From the Radcliffe Department of Medicine, Acute Vascular Imaging Centre (G.W.J.H., D.C., F.S., J.K.)
From the Radcliffe Department of Medicine, Acute Vascular Imaging Centre (G.W.J.H., D.C., F.S., J.K.).
Stroke. 2018 Jul;49(7):1647-1655. doi: 10.1161/STROKEAHA.118.020788. Epub 2018 Jun 12.
Lesion expansion in the week after acute stroke involves both infarct growth (IG) and anatomic distortion (AD) because of edema and hemorrhage. Enabling separate quantification would allow clinical trials targeting these distinct pathological processes. We developed an objective and automated approach to quantify these processes at 24 hours and 1 week.
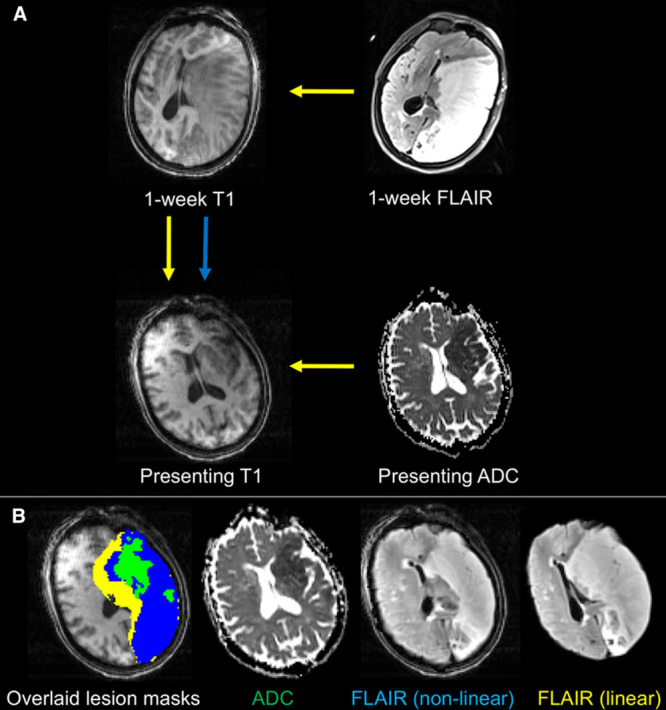
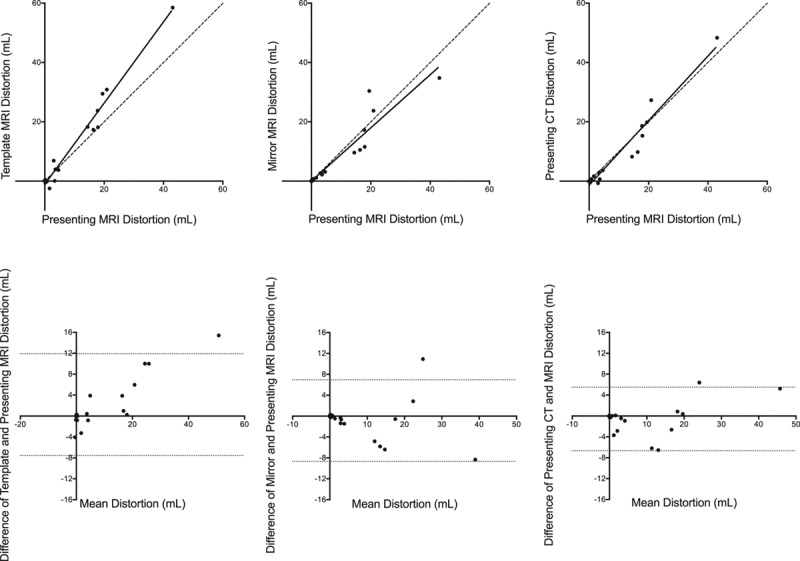
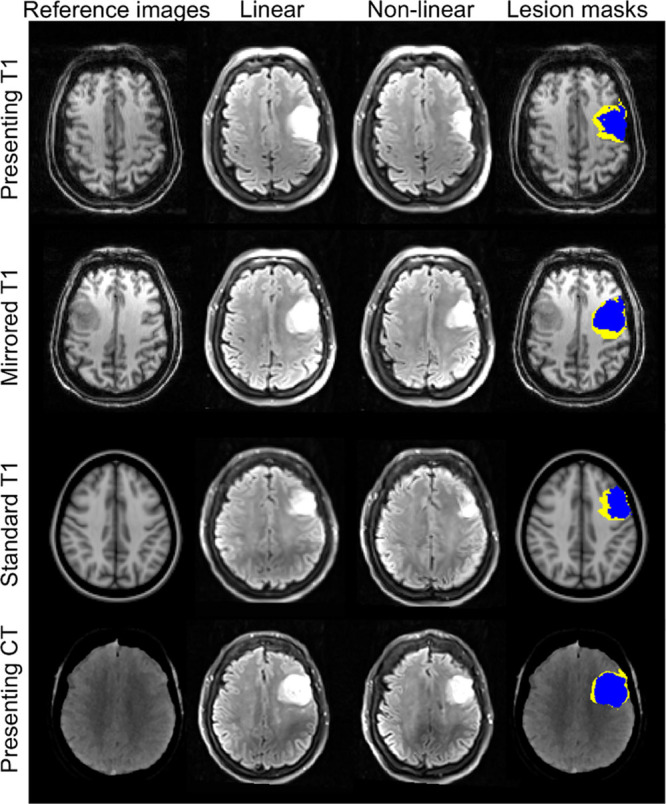
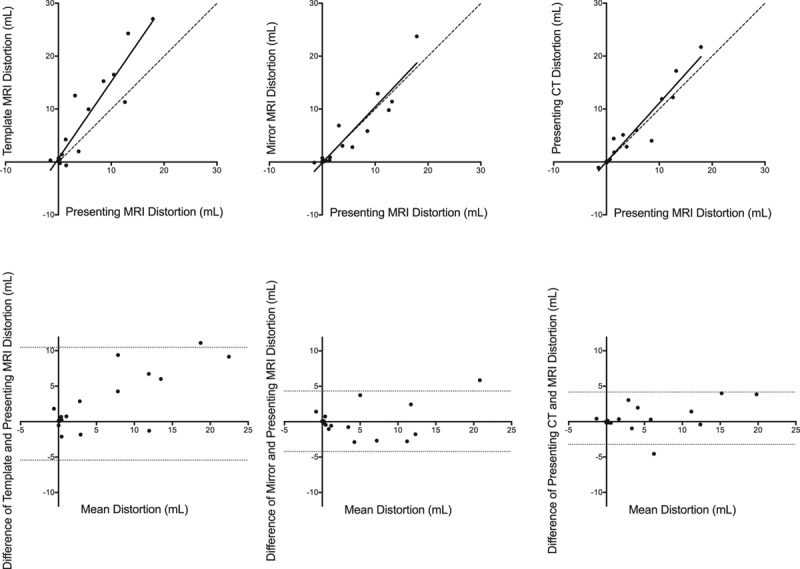
Patients with acute ischemic stroke were scanned at presentation, 24 hours, and 1 week in a magnetic resonance imaging (MRI) cohort study. IG and AD were calculated from follow-up lesion masks after linear and nonlinear registration to a presenting MRI scan. Performance of IG and AD was compared with edema quantified using cerebrospinal fluid displacement. The use of alternative reference images to define AD, including template MRI, mirrored MRI, and presenting computed tomographic scan, was explored.
Thirty-seven patients with nonlacunar stroke were included. AD was responsible for 20% and 36% of lesion expansion at 24 hours (n=30) and 1 week (n=28). Registration-defined IG and AD compared favorably with edema quantified using cerebrospinal fluid displacement, particularly at smaller infarct volumes. Presenting computed tomographic imaging was the preferred alternative reference image to presenting MRI for measuring AD.
The contributions of IG and AD to lesion expansion can be measured separately over time through the use of image registration. This approach can be used to combine imaging outcome data from computed tomography and MRI.
急性卒中后一周内的病灶扩大包括梗死生长(IG)和由于水肿和出血导致的解剖变形(AD)。能够对这两种过程进行单独定量将允许临床试验针对这些不同的病理过程。我们开发了一种客观且自动化的方法,可在 24 小时和 1 周时定量测量这两种过程。
在一项磁共振成像(MRI)队列研究中,对急性缺血性卒中患者在发病时、24 小时和 1 周时进行扫描。IG 和 AD 通过从后续病变掩模到初始 MRI 扫描的线性和非线性配准进行计算。将 IG 和 AD 的性能与使用脑脊液位移定量的水肿进行了比较。还探索了使用替代参考图像(包括模板 MRI、镜像 MRI 和初始 CT 扫描)来定义 AD。
共纳入 37 例非腔隙性卒中患者。在 24 小时(n=30)和 1 周(n=28)时,AD 分别导致 20%和 36%的病灶扩大。通过图像配准定义的 IG 和 AD 与使用脑脊液位移定量的水肿具有良好的可比性,特别是在较小的梗死体积时。与初始 MRI 相比,初始 CT 成像作为 AD 的替代参考图像更为可取。
通过使用图像配准,可以随时间分别测量 IG 和 AD 对病灶扩大的贡献。该方法可用于结合 CT 和 MRI 的成像结果数据。