Tanzania Field Epidemiology and Laboratory Training Program, Ministry of Health, Community Development, Gender, Elderly and Children, P.O Box 71286, Ocean Road, Dar es Salaam, Tanzania.
Department of Microbiology and Immunology, Muhimbili University of Health and Allied Science, Dar es Salaam, Tanzania.
BMC Infect Dis. 2018 Jun 14;18(1):276. doi: 10.1186/s12879-018-3183-9.
In the past two decades, Rift Valley Fever (RVF) outbreaks have been reported twice in Tanzania, with the most recent outbreak occurring in 2006/07. Given the ecology and climatic factors that support mosquito vectors in the Serengeti ecosystem, we hypothesized a continued transmission of RVF virus (RVFV) during interepidemic periods. This study was carried out to determine sero-prevalence, spatial distribution and factors associated with RVF in at-risk agro-pastoral and pastoral communities in the Serengeti Ecosystem in northern Tanzania.
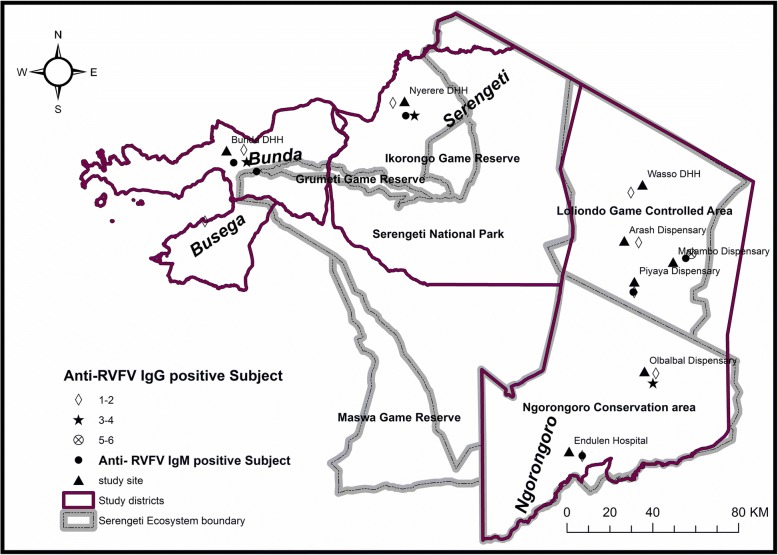
A cross sectional study was carried out to establish the general exposure to RVFV by detecting anti-RVFV IgG and anti-RVFV IgM using ELISA techniques. The health facilities where human subjects were blood sampled concurrent with interviews included Bunda District Designated Hospital, Wasso DDH, Endulen hospital, Arash, Malambo, Olbabal, and Piyaya dispenaries (Ngorongoro district) and Nyerere DDH (Serengeti district) respectively. In addition, human subjects from Lamadi ward (Busega district) were recruited while receiving medical service at Bunda DDH. We conducted logistic regression to assess independent risk factor and mapped the hotspot areas for exposure to RVFV.
A total of 751 subjects (males = 41.5%; females = 58.5%) with a median age of 35.5 years were enrolled at out-patient clinics. Of them, 34 (4.5, 95%CI 3.3-6.3%) tested positive for anti-RVFV IgG. Of the 34 that tested positive for anti-RVFV IgG, six (17.6%) tested positive for anti-RVFV IgM. Odds of exposure were higher among pastoral communities (aOR 2.9, 95% C.I: 1.21-6.89, p < 0.01), and agro-pastoral communities residing in Ngorongoro District (aOR 1.8, 95% C.I 1.14-3.39, p = 0.03). Hotspot areas for exposure to RVFV were Malambo, Olbalbal and Piyaya wards in Ngorongoro district, and Lamadi ward in Busega district.
The study found both previous and recent exposure of RVFV in humans residing in the Serengeti ecosystem as antibodies against both IgG and IgM were detected. Detection of anti-RVF IgM suggests an ongoing transmission of RVFV in humans during inter-epidemic periods. Residents of Ngorongoro district were most exposed to RVFV compared to Bunda and Serengeti districts. Therefore, the risk of exposure to RVFV was higher among pastoral communities compared to farming communities.
在过去的二十年中,裂谷热(RVF)在坦桑尼亚爆发了两次,最近一次爆发发生在 2006/07 年。鉴于支持塞伦盖蒂生态系统中蚊子传播媒介的生态和气候因素,我们假设 RVF 病毒(RVFV)在流行间歇期仍在持续传播。本研究旨在确定坦桑尼亚北部塞伦盖蒂生态系统中处于危险中的农牧社区中 RVF 的血清流行率、空间分布和相关因素。
采用酶联免疫吸附试验(ELISA)技术检测抗 RVFV IgG 和抗 RVFV IgM,进行横断面研究,以确定 RVFV 的一般暴露情况。进行人类抽样的卫生设施包括邦达区指定医院、Wasso DDH、恩杜伦医院、阿拉什、马兰博、奥巴尔巴尔和皮亚亚诊所(恩戈罗恩戈罗区)和尼雷尔 DDH(塞伦盖蒂区)。此外,在邦达 DDH 接受医疗服务的同时,还从拉马迪病房(布塞加区)招募了人类受试者。我们进行逻辑回归分析,以评估独立的危险因素,并绘制 RVFV 暴露的热点区域图。
共有 751 名受试者(男性占 41.5%;女性占 58.5%),中位年龄为 35.5 岁,在门诊接受了检查。其中,34 名(4.5%,95%CI 3.3-6.3%)检测出抗 RVFV IgG 呈阳性。在 34 名抗 RVFV IgG 呈阳性的受试者中,有 6 名(17.6%)抗 RVFV IgM 呈阳性。牧民社区(优势比 2.9,95%置信区间:1.21-6.89,p<0.01)和居住在恩戈罗恩戈罗区的农牧社区(优势比 1.8,95%置信区间:1.14-3.39,p=0.03)的暴露几率更高。RVFV 暴露的热点区域是恩戈罗恩戈罗区的马兰博、奥巴尔巴尔和皮亚亚病房,以及布塞加区的拉马迪病房。
本研究发现,居住在塞伦盖蒂生态系统中的人类既存在既往 RVFV 暴露,也存在近期 RVFV 暴露,因为检测到了 IgG 和 IgM 抗体。抗 RVFV IgM 的检测表明,在流行间歇期,RVFV 仍在人类中持续传播。与邦达和塞伦盖蒂区相比,恩戈罗恩戈罗区的居民接触 RVFV 的风险更高。因此,与农耕社区相比,牧民社区接触 RVFV 的风险更高。