Department of Laboratory Medicine and Pathology, Mayo Clinic, Rochester, MN
Division of Biomedical Statistics and Informatics, Mayo Clinic, Rochester, MN.
Haematologica. 2018 Nov;103(11):1899-1907. doi: 10.3324/haematol.2018.190157. Epub 2018 Jun 14.
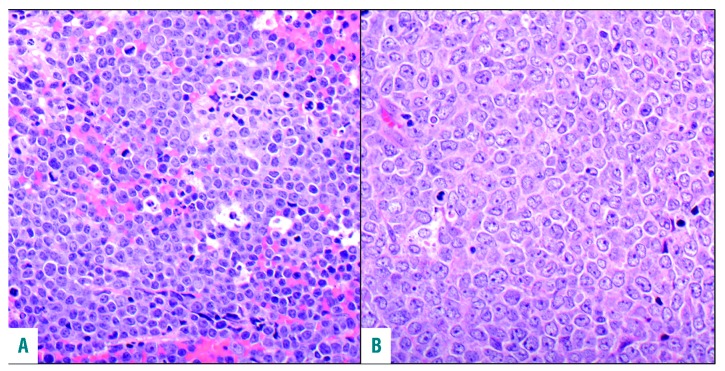
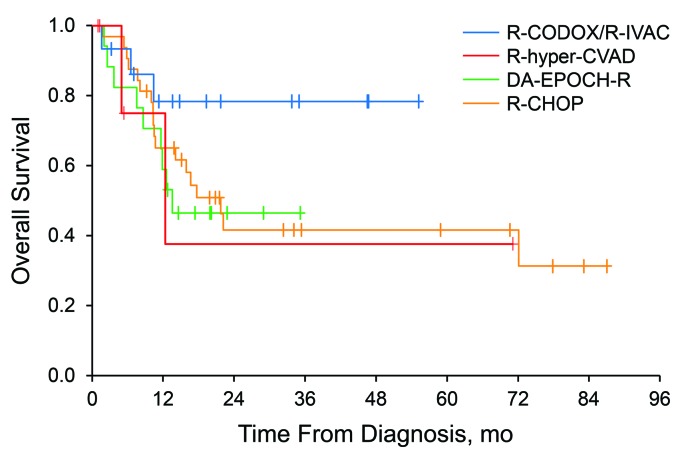
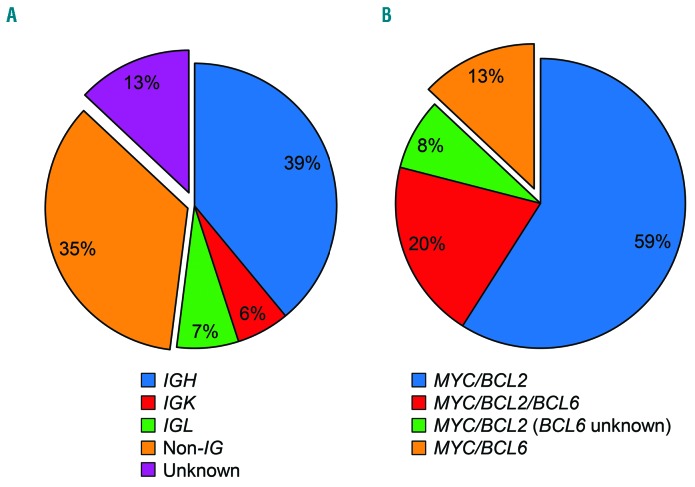
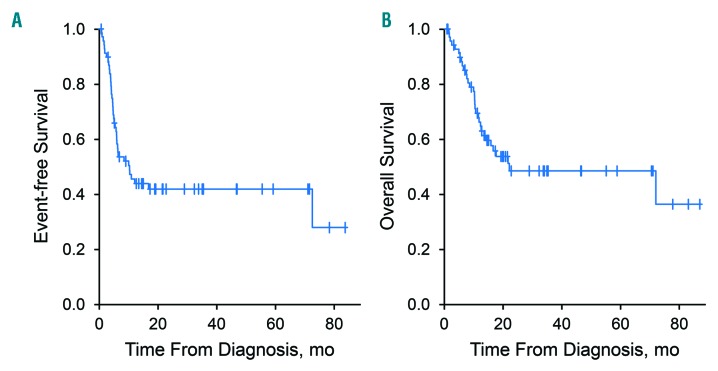
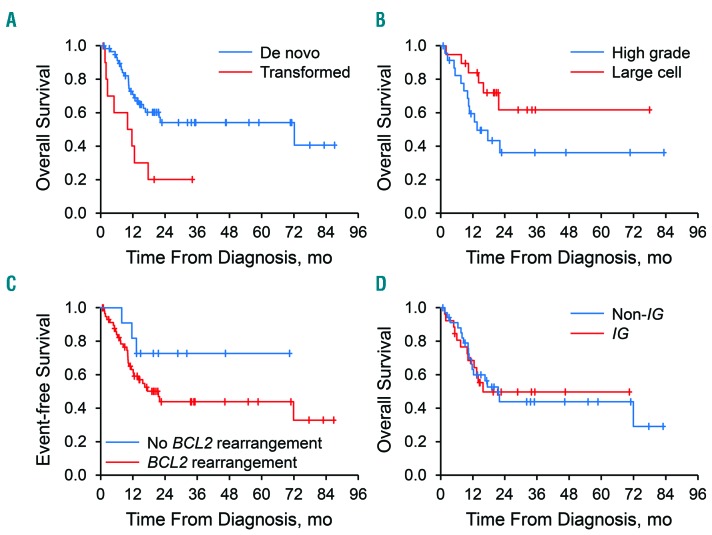
High-grade B-cell lymphomas with and and/or rearrangements (double-/triple-hit lymphoma) have an aggressive clinical course. We investigated the prognostic value of transformation from low-grade lymphoma, cytological features (high grade large cell), rearrangement partners (immunoglobulin nonimmunoglobulin gene), and treatment. We evaluated 100 adults with double-/triple-hit lymphoma, reviewing cytological features; cell of origin; and rearrangements of , , and using , , and break-apart and , , , and dual-fusion interphase fluorescence hybridization probes. Outcome analysis was restricted to patients with lymphoma, or at transformation, who received anthracycline-based chemotherapy. Among them, 60% had high-grade cytological features; 91% had a germinal center B-cell phenotype, and 60% had a rearrangement. Germinal center B-cell phenotype was associated with rearrangements (<0.001). Mean (95% confidence interval) 5-year overall survival was 49% (37%-64%). Transformation from previously treated and untreated low-grade lymphoma was associated with inferior overall survival (hazard ratio, 2.99; =0.008). Patients with high-grade cytological features showed a non-significant tendency to inferior outcome (hazard ratio, 2.32; =0.09). No association was observed between rearrangement partner and overall survival (hazard ratio, 1.00; =0.99). Compared with patients receiving rituximab, cyclophosphamide, doxorubicin, and vincristine (R-CHOP) and dose-adjusted etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin, and rituximab (EPOCH-R), patients receiving rituximab, cyclophosphamide, vincristine, doxorubicin, methotrexate/ifosfamide, etoposide, and cytarabine (R-CODOX-M/IVAC) had a non-significant tendency to better overall survival (hazard ratio, 0.37; =0.10). In conclusion, high-grade B-cell lymphomas with and and/or rearrangements had heterogeneous outcomes and rearrangements were not associated with inferior overall survival.
具有 和/或 重排的高级别 B 细胞淋巴瘤(双-/三打击淋巴瘤)具有侵袭性的临床病程。我们研究了从低级别淋巴瘤转化、细胞学特征(高级别大细胞)、重排伙伴(免疫球蛋白非免疫球蛋白基因)以及治疗的预后价值。我们评估了 100 名双-/三打击淋巴瘤成人患者,通过使用 、 、 和 断裂分离和 、 、 、 和 双重融合间期荧光杂交探针,回顾了细胞学特征;细胞起源;和 、 、 和 的重排。结果分析仅限于在转化为淋巴瘤、或时接受基于蒽环类药物的化疗的患者。其中,60%的患者具有高级别的细胞学特征;91%的患者具有生发中心 B 细胞表型,60%的患者具有 重排。生发中心 B 细胞表型与 重排相关(<0.001)。5 年总生存率的平均值(95%置信区间)为 49%(37%-64%)。先前治疗和未治疗的低级别淋巴瘤转化与总生存率降低相关(风险比,2.99;=0.008)。具有高级别细胞学特征的患者表现出非显著的预后不良趋势(风险比,2.32;=0.09)。重排伙伴与总生存率之间未观察到相关性(风险比,1.00;=0.99)。与接受利妥昔单抗、环磷酰胺、多柔比星和长春新碱(R-CHOP)和剂量调整依托泊苷、泼尼松、长春新碱、环磷酰胺、多柔比星和利妥昔单抗(EPOCH-R)的患者相比,接受利妥昔单抗、环磷酰胺、长春新碱、多柔比星、甲氨蝶呤/异环磷酰胺、依托泊苷和阿糖胞苷(R-CODOX-M/IVAC)的患者总生存率有非显著的改善趋势(风险比,0.37;=0.10)。总之,具有 和/或 重排的高级别 B 细胞淋巴瘤具有异质性结局,且 重排与总生存率降低无关。