Department of Anaesthesiology and Intensive Care Medicine, University Hospital of Bonn, Bonn, Germany.
Department of Radiology, University Hospital of Bonn, Bonn, Germany.
J Cardiovasc Magn Reson. 2018 Jun 18;20(1):40. doi: 10.1186/s12968-018-0455-x.
Prolonged breath holding results in hypoxemia and hypercapnia. Compensatory mechanisms help maintain adequate oxygen supply to hypoxia sensitive organs, but burden the cardiovascular system. The aim was to investigate human compensatory mechanisms and their effects on the cardiovascular system with regard to cardiac function and morphology, blood flow redistribution, serum biomarkers of the adrenergic system and myocardial injury markers following prolonged apnoea.
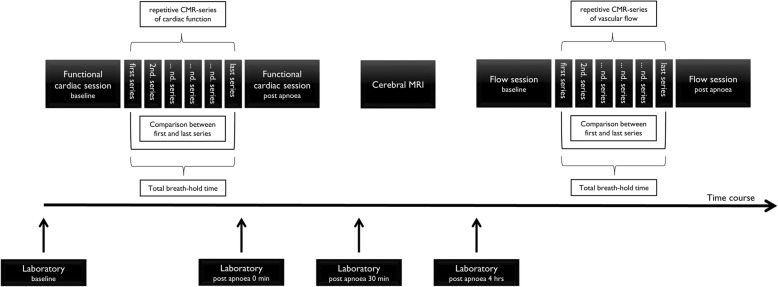
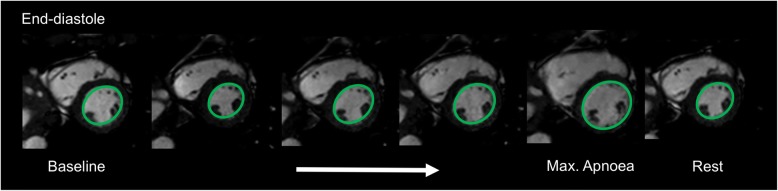
Seventeen elite apnoea divers performed maximal breath-hold during cardiovascular magnetic resonance imaging (CMR). Two breath-hold sessions were performed to assess (1) cardiac function, myocardial tissue properties and (2) blood flow. In between CMR sessions, a head MRI was performed for the assessment of signs of silent brain ischemia. Urine and blood samples were analysed prior to and up to 4 h after the first breath-hold.
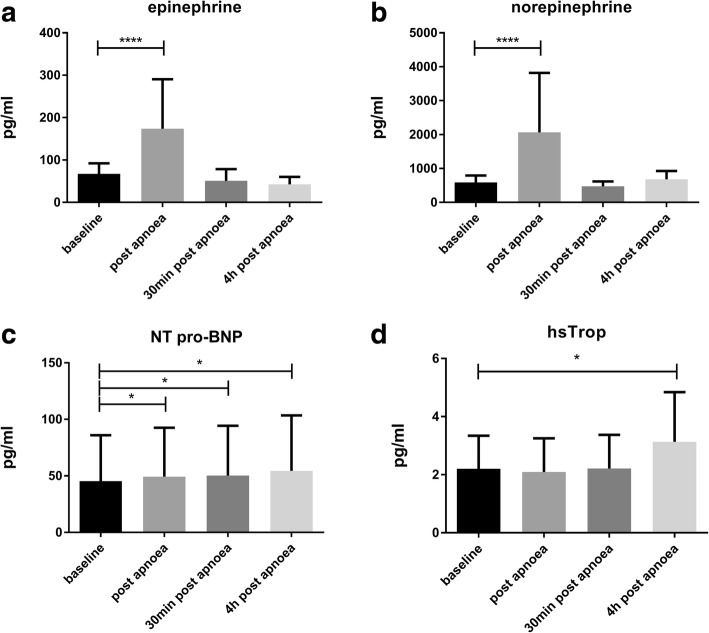
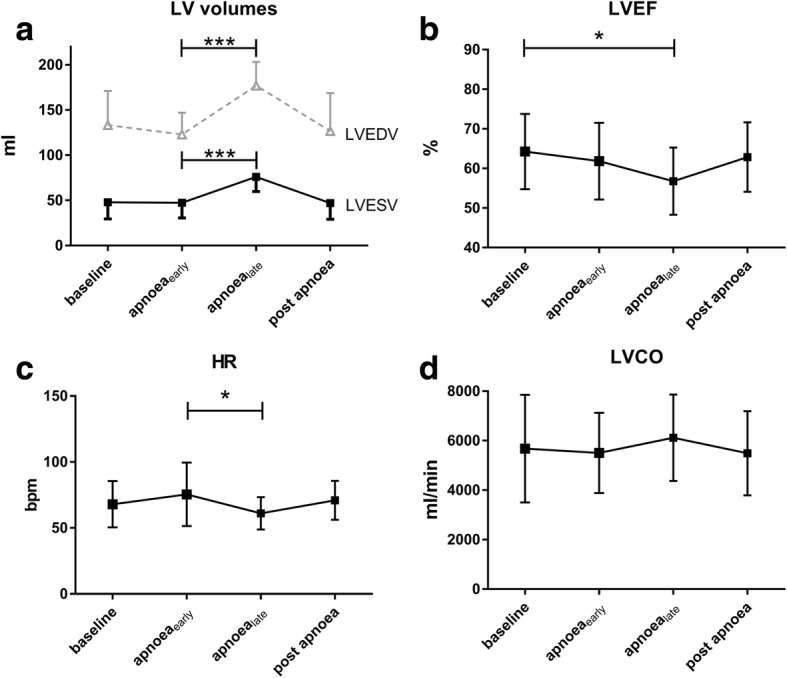
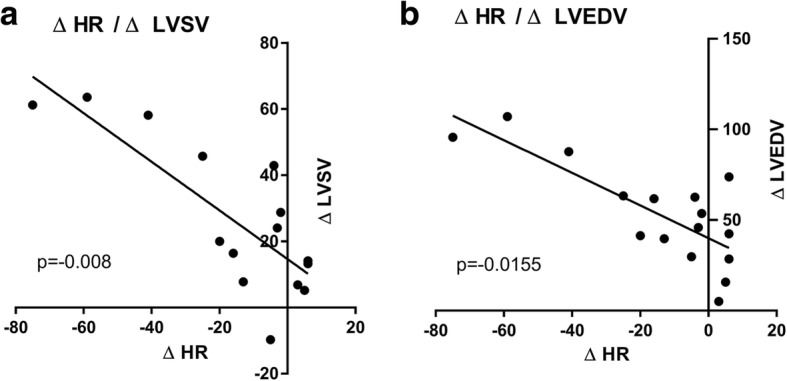
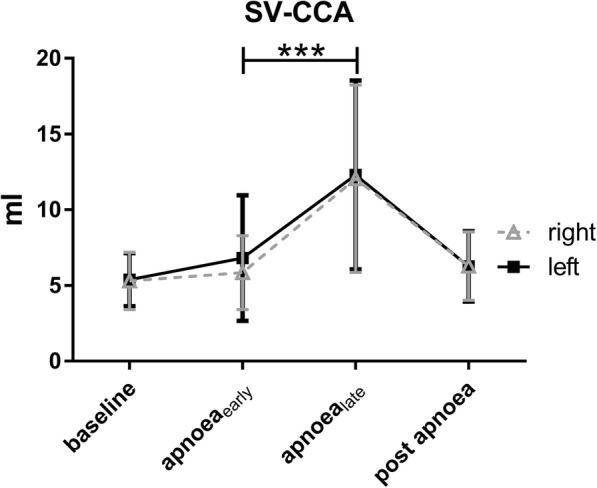
Mean breath-hold time was 297 ± 52 s. Left ventricular (LV) end-systolic, end-diastolic, and stroke volume increased significantly (p < 0.05). Peripheral oxygen saturation, LV ejection fraction, LV fractional shortening, and heart rate decreased significantly (p < 0.05). Blood distribution was diverted to cerebral regions with no significant changes in the descending aorta. Catecholamine levels, high-sensitivity cardiac troponin, and NT-pro-BNP levels increased significantly, but did not reach pathological levels.
Compensatory effects of prolonged apnoea substantially burden the cardiovascular system. CMR tissue characterisation did not reveal acute myocardial injury, indicating that the resulting cardiovascular stress does not exceed compensatory physiological limits in healthy subjects. However, these compensatory mechanisms could overly tax those limits in subjects with pre-existing cardiac disease. For divers interested in competetive apnoea diving, a comprehensive medical exam with a special focus on the cardiovascular system may be warranted.
This prospective single-centre study was approved by the institutional ethics committee review board. It was retrospectively registered under ClinicalTrials.gov (Trial registration: NCT02280226 . Registered 29 October 2014).
长时间的屏气会导致低氧血症和高碳酸血症。代偿机制有助于维持缺氧敏感器官的充足氧气供应,但会给心血管系统带来负担。目的是研究人体代偿机制及其对心血管系统的影响,包括心脏功能和形态、血流再分布、儿茶酚胺系统的血清生物标志物和心肌损伤标志物,以评估长时间屏气后的变化。
17 名精英 apnea 潜水员在心血管磁共振成像(CMR)期间进行最大程度的屏气。进行了两次屏气测试,以评估(1)心脏功能、心肌组织特性和(2)血流。在 CMR 测试之间,进行头部 MRI 以评估无症状性脑缺血的迹象。在第一次屏气前和屏气后 4 小时内分析尿液和血液样本。
平均屏气时间为 297±52 秒。左心室(LV)收缩末期、舒张末期和心搏量显著增加(p<0.05)。外周血氧饱和度、LV 射血分数、LV 缩短分数和心率显著降低(p<0.05)。血液分布被转移到脑部区域,降主动脉没有明显变化。儿茶酚胺水平、高敏心肌肌钙蛋白和 NT-pro-BNP 水平显著升高,但未达到病理水平。
长时间屏气的代偿效应对心血管系统造成了很大的负担。CMR 组织特征没有显示出急性心肌损伤,这表明在健康受试者中,由此产生的心血管压力没有超过代偿性生理极限。然而,这些代偿机制可能会使那些有预先存在的心脏疾病的人过度超过这些极限。对于有兴趣参加竞技 apnea 潜水的潜水员,可能需要进行全面的医学检查,特别是要关注心血管系统。
这是一项前瞻性单中心研究,得到了机构伦理委员会的批准。它在 ClinicalTrials.gov 上进行了回顾性注册(试验注册:NCT02280226。注册日期:2014 年 10 月 29 日)。