National Institute of Health (NIH) / National Institute of Neurological Disorders and Stroke (NINDS), Bethesda, MD, USA.
Department of Radiology, University Medical Centre Utrecht, Utrecht, The Netherlands.
Neuroimage. 2018 Oct 1;179:530-539. doi: 10.1016/j.neuroimage.2018.06.017. Epub 2018 Jun 18.
The BOLD signal amplitude as a response to a hypercapnia stimulus is commonly used to assess cerebrovascular reserve. Despite recent advances, the implementation remains cumbersome and alternative ways to assess hemodynamic impairment are desirable. Resting-state BOLD signal fluctuations (rsBOLD) have been proposed however data on its sensitivity and dependence on baseline venous cerebral blood volume (vCBV) is limited. The primary aim of this study was to compare the effect sizes of resting-state and hypercapnia induced BOLD signal changes in the detection of hemodynamic impairment. The second aim of the study was to assess the dependence of BOLD signal variability on vCBV.
Fifteen patients with internal carotid artery occlusive disease and 15 matched healthy controls were included in this study. The BOLD signal was derived from a dual-echo gradient-echo echo-planar sequence during hypercapnia (HC) and hyperoxia (HO) gas modulations. BOLD (fractional) amplitude of low frequency fluctuations ((f)ALFF) was compared to HC-BOLD, BOLD response delays derived from time delay analysis and ΔBOLD in response to progressively increasing HC. Effect sizes (i.e. the standard mean difference between patients and controls) were calculated. HO-BOLD was used to estimate vCBV, and its contribution to the variability in rsBOLD signal was evaluated.
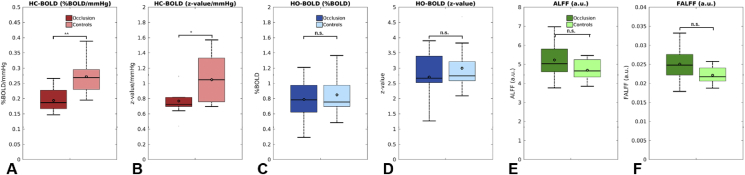
The effect sizes of ALFF and fALFF (0.61 and 0.72) were lower than the effect sizes related to hypercapnia-based hemodynamic assessment analysis; 1.62, 1.56 and 0.90 for HC-BOLD, BOLD response delays and ΔBOLD in response to progressively increasing HC. A moderate relation was found between (f)ALFF and HC-BOLD in controls (R of 0.61 and 0.42), but this relation decreased in patients (R of 0.33 and 0.15). (f)ALFF did not differ between patients and controls whereas HC-BOLD did (p < 0.005). The ΔBOLD response to progressively increasing HC was significantly different in between patients and controls for ΔEtCO values ≥ 2 mmHg (at +2 mmHg F(1, 18) = 5.85, p = 0.026). Up to 31% and 53% of the variance in the ALFF and HC-BOLD spatial distribution could be explained by HO-BOLD.
ALFF and fALFF demonstrated a moderate effect size to detect hemodynamic impairment whereas the effect size was large for methods employing a hypercapnia-based vascular stress stimulus. Based on our analysis of BOLD signal change as a response to a progressively increasing hypercapnia stimulus we can argue that a hypercapnia stimulus of at least 2 mmHg above baseline EtCO is necessary to evaluate hemodynamic impairment. We also demonstrated that a substantial amount of information imbedded in the rsBOLD and HC-BOLD was explained by HO-BOLD. HO-BOLD can serve as a proxy for vCBV and this thus indicates that one should be careful when adopting these techniques in disease cases with compromised CBV.

作为对高碳酸血症刺激的反应,BOLD 信号幅度通常用于评估脑血管储备。尽管最近取得了进展,但实施仍然很繁琐,需要替代方法来评估血液动力学损伤。然而,静息态 BOLD 信号波动(rsBOLD)已经被提出,但其对基线静脉脑血容量(vCBV)的敏感性和依赖性的数据有限。本研究的主要目的是比较静息态和高碳酸血症诱导的 BOLD 信号变化在检测血液动力学损伤方面的效果大小。本研究的第二个目的是评估 BOLD 信号变异性对 vCBV 的依赖性。
本研究纳入了 15 例颈内动脉闭塞性疾病患者和 15 例匹配的健康对照者。在高碳酸血症(HC)和高氧(HO)气体调制期间,从双回波梯度回波 EPI 序列中获得 BOLD 信号。比较低频率波动(f)ALFF 与 HC-BOLD、源自时间延迟分析的 BOLD 反应延迟以及与逐渐增加的 HC 对应的 ΔBOLD。计算效应大小(即患者和对照组之间的标准平均差异)。使用 HO-BOLD 来估计 vCBV,并评估其对 rsBOLD 信号变异性的贡献。
ALFF 和 fALFF 的效应大小(0.61 和 0.72)低于基于高碳酸血症的血液动力学评估分析的效应大小;1.62、1.56 和 0.90 分别为 HC-BOLD、BOLD 反应延迟和与逐渐增加的 HC 对应的 ΔBOLD。在对照组中,(f)ALFF 与 HC-BOLD 之间存在中度相关性(R 为 0.61 和 0.42),但在患者中,这种相关性降低(R 为 0.33 和 0.15)。(f)ALFF 在患者和对照组之间没有差异,而 HC-BOLD 有差异(p<0.005)。对于 ΔEtCO 值≥2mmHg 的逐渐增加的 HC 的 ΔBOLD 反应,患者和对照组之间存在显著差异(在+2mmHg 时 F(1, 18)=5.85,p=0.026)。ALFF 和 HC-BOLD 空间分布的方差可以用 HO-BOLD 解释高达 31%和 53%。
ALFF 和 fALFF 表现出中等的检测血液动力学损伤的效果大小,而采用基于高碳酸血症的血管应激刺激的方法则具有较大的效果大小。基于我们对作为逐渐增加的高碳酸血症刺激的反应的 BOLD 信号变化的分析,我们可以认为,需要至少 2mmHg 以上的基础 EtCO 的高碳酸血症刺激来评估血液动力学损伤。我们还证明了 rsBOLD 和 HC-BOLD 中嵌入的大量信息可以用 HO-BOLD 来解释。HO-BOLD 可以作为 vCBV 的替代物,因此这表明在 CBV 受损的疾病情况下采用这些技术时应该小心。