Johns Hopkins Bloomberg School of Public Health and Johns Hopkins University, Baltimore, Maryland (E.S., D.W., K.M., M.E.G., J.C.).
Ann Intern Med. 2018 Aug 7;169(3):156-164. doi: 10.7326/M18-0091. Epub 2018 Jun 19.
Current clinical definitions of diabetes require repeated blood work to confirm elevated levels of glucose or hemoglobin A1c (HbA1c) to reduce the possibility of a false-positive diagnosis. Whether 2 different tests from a single blood sample provide adequate confirmation is uncertain.
To examine the prognostic performance of a single-sample confirmatory definition of undiagnosed diabetes.
Prospective cohort study.
The ARIC (Atherosclerosis Risk in Communities) study.
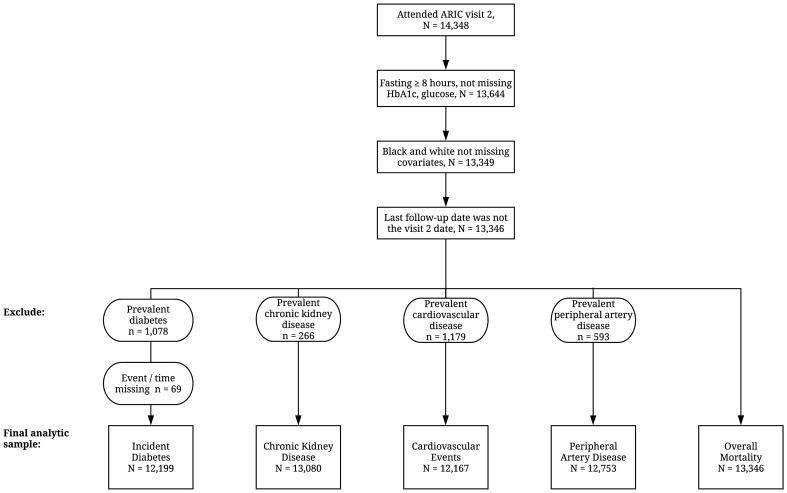
13 346 ARIC participants (12 268 without diagnosed diabetes) with 25 years of follow-up for incident diabetes, cardiovascular outcomes, kidney disease, and mortality.
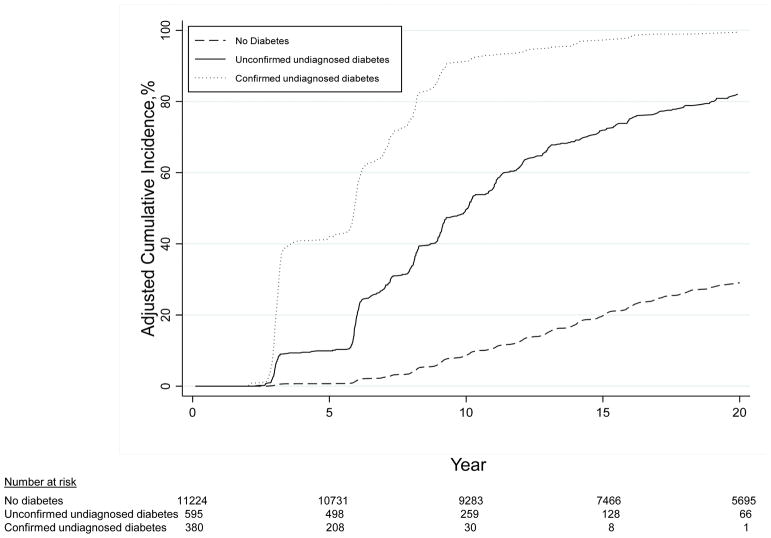
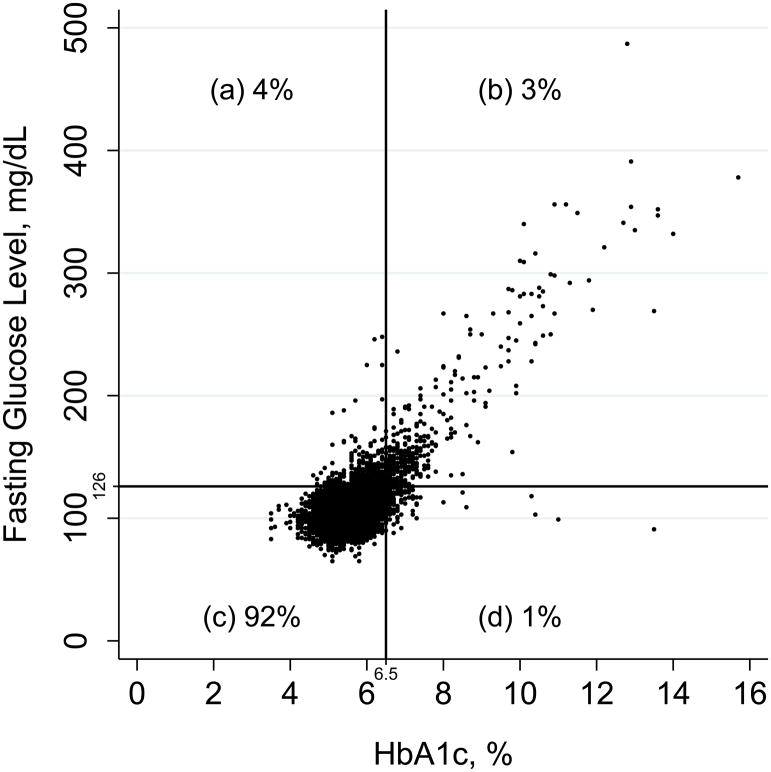
Confirmed undiagnosed diabetes was defined as elevated levels of fasting glucose (≥7.0 mmol/L [≥126 mg/dL]) and HbA1c (≥6.5%) from a single blood sample.
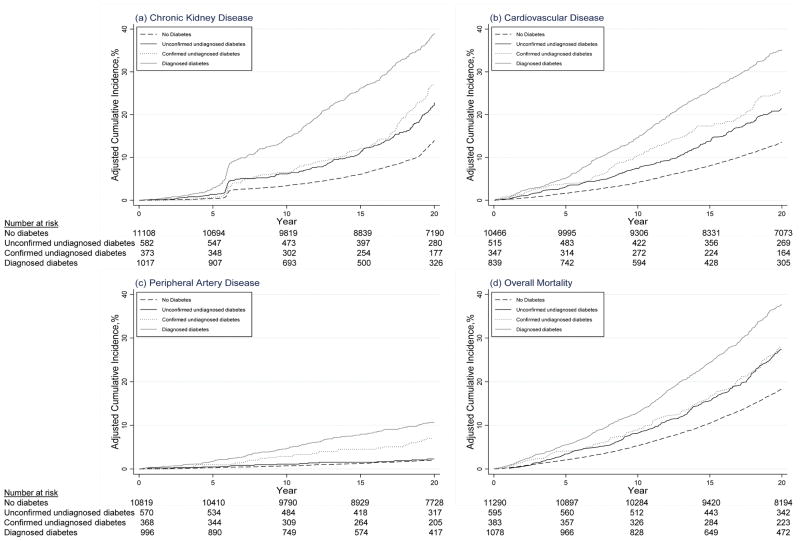
Among 12 268 participants without diagnosed diabetes, 978 had elevated levels of fasting glucose or HbA1c at baseline (1990 to 1992). Among these, 39% had both (confirmed undiagnosed diabetes), whereas 61% had only 1 elevated measure (unconfirmed undiagnosed diabetes). The confirmatory definition had moderate sensitivity (54.9%) but high specificity (98.1%) for identification of diabetes cases diagnosed during the first 5 years of follow-up, with specificity increasing to 99.6% by 15 years. The 15-year positive predictive value was 88.7% compared with 71.1% for unconfirmed cases. Confirmed undiagnosed diabetes was significantly associated with cardiovascular and kidney disease and mortality, with stronger associations than unconfirmed diabetes.
Lack of repeated measurements of fasting glucose and HbA1c.
A single-sample confirmatory definition of diabetes had a high positive predictive value for subsequent diagnosis and was strongly associated with clinical end points. Our results support the clinical utility of using a combination of elevated fasting glucose and HbA1c levels from a single blood sample to identify undiagnosed diabetes in the population.
National Institute of Diabetes and Digestive and Kidney Diseases and National Heart, Lung, and Blood Institute.
目前,糖尿病的临床诊断需要通过重复的血液检查来确认血糖或糖化血红蛋白(HbA1c)水平升高,以降低假阳性诊断的可能性。单次血样中进行两项不同检查是否足以确认仍不确定。
检验单次样本确认法对未确诊糖尿病的预测价值。
前瞻性队列研究。
ARIC(社区动脉粥样硬化风险)研究。
ARIC 研究共纳入 13346 名参与者(12268 名无糖尿病诊断),平均随访 25 年,随访终点为新发糖尿病、心血管结局、肾脏疾病和死亡。
确诊的未确诊糖尿病定义为单次血样中空腹血糖(≥7.0mmol/L[≥126mg/dL])和糖化血红蛋白(≥6.5%)升高。
在 12268 名无糖尿病诊断的参与者中,978 名基线时(1990 至 1992 年)空腹血糖或糖化血红蛋白升高(未确诊糖尿病)。其中,39%的患者同时存在两项升高指标(确诊的未确诊糖尿病),61%的患者仅存在 1 项升高指标(未确诊的未确诊糖尿病)。该确认性诊断标准对随访前 5 年确诊的糖尿病病例具有中等敏感性(54.9%)和高特异性(98.1%),特异性在随访 15 年后提高至 99.6%。15 年阳性预测值为 88.7%,而未确诊病例为 71.1%。确诊的未确诊糖尿病与心血管和肾脏疾病及死亡率显著相关,与未确诊的糖尿病相比,其相关性更强。
缺乏空腹血糖和糖化血红蛋白的重复测量。
糖尿病的单次样本确认性定义对后续诊断具有较高的阳性预测值,与临床终点有较强的关联。我们的研究结果支持使用单次血样中升高的空腹血糖和糖化血红蛋白水平组合来识别人群中的未确诊糖尿病的临床实用性。
美国国立糖尿病、消化和肾脏疾病研究所和美国国立心肺血液研究所。