Winthereik Anna Kirstine, Neergaard Mette Asbjoern, Jensen Anders Bonde, Vedsted Peter
Department of Oncology, Aarhus University Hospital, Noerrebrogade 44, 8000, Aarhus C, Denmark.
Department of Clinical Medicine, Aarhus University, Noerrebrogade 44, 8000, Aarhus C, Denmark.
BMC Fam Pract. 2018 Jun 20;19(1):91. doi: 10.1186/s12875-018-0774-x.
Most patients in end-of-life with life-threatening diseases prefer to be cared for and die at home. Nevertheless, the majority die in hospitals. GPs have a pivotal role in providing end-of-life care at patients' home, and their involvement in the palliative trajectory enhances the patient's possibility to stay at home. The aim of this study was to develop and pilot-test an intervention consisting of continuing medical education (CME) and electronic decision support (EDS) to support end-of-life care in general practice.
We developed an intervention in line with the first phases of the guidelines for complex interventions drawn up by the Medical Research Council. Phase 1 involved the development of the intervention including identification of key barriers to provision of end-of-life care for GPs and of facilitators of change. Furthermore the actual modelling of two components: CME meeting and EDS. Phase 2 focused on pilot-testing and intervention assessment by process evaluation.
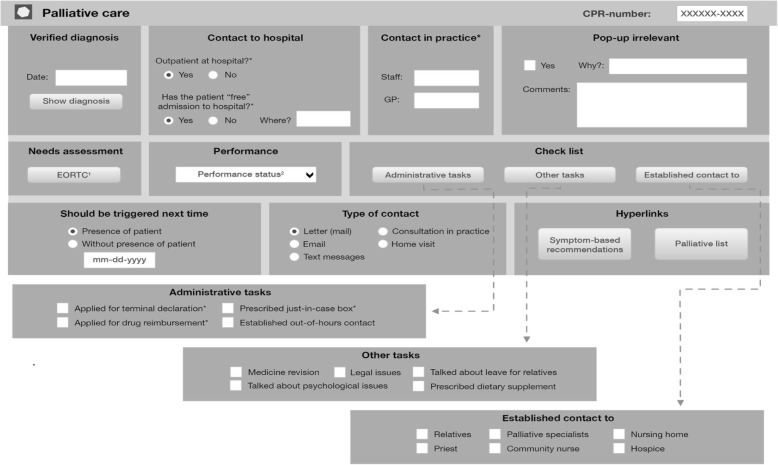
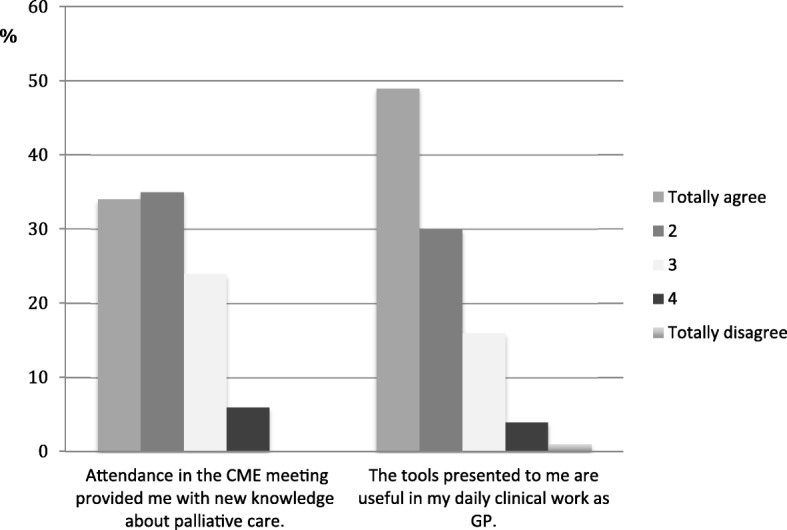
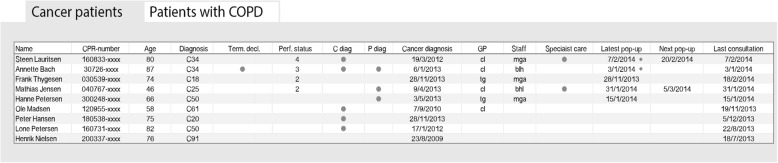
In phase 1 lack of identification of patients at the end of life and limited palliative knowledge among GPs were identified as barriers. The CME meeting and the EDS were developed. The CME meeting was a four-hour educational meeting performed by GPs and specialists in palliative care. The EDS consisted of two parts: a pop-up window for each patient with palliative needs and a list of all patients with palliative needs in the practice. The pilot testing in phase 2 showed that the CME meeting was performed as intended and 120 (14%) of the GPs in the region attended. The EDS was integrated in existing electronic records but was shut down early for external reasons; 50 (5%) GPs signed up. The pilot-testing demonstrated a need to strengthen the implementation as attending rate was low in the current set-up.
We developed a complex intervention to support GPs in providing end-of-life care. The pilot-test showed general acceptance of the CME meetings. The EDS was shut down early and needs further evaluation before examining the whole intervention in a larger study, where evaluation could be based on patient-related outcomes and impact on end-of-life care.
Clinicaltrials.gov ( NCT02050256 ) January 30, 2014.
大多数患有危及生命疾病的临终患者更愿意在家中接受护理并离世。然而,大多数患者却在医院死亡。全科医生在为患者在家中提供临终护理方面发挥着关键作用,他们参与姑息治疗轨迹可提高患者在家中离世的可能性。本研究的目的是开发并进行一项由继续医学教育(CME)和电子决策支持(EDS)组成的干预措施,以支持全科医疗中的临终护理。
我们根据医学研究理事会制定的复杂干预指南的第一阶段开发了一项干预措施。第一阶段包括干预措施的开发,包括确定全科医生提供临终护理的关键障碍和变革促进因素。此外,还对两个组成部分进行了实际建模:CME会议和EDS。第二阶段侧重于通过过程评估进行试点测试和干预评估。
在第一阶段,确定了临终患者识别不足和全科医生姑息治疗知识有限是障碍。开发了CME会议和EDS。CME会议是由全科医生和姑息治疗专家举办的为期四小时的教育会议。EDS由两部分组成:为每位有姑息治疗需求的患者弹出的窗口以及诊所中所有有姑息治疗需求患者的列表。第二阶段的试点测试表明,CME会议按计划进行,该地区120名(14%)全科医生参加。EDS已整合到现有的电子记录中,但因外部原因提前关闭;50名(5%)全科医生报名。试点测试表明需要加强实施,因为在当前设置下参与率较低。
我们开发了一项复杂干预措施以支持全科医生提供临终护理。试点测试表明CME会议得到了普遍认可。EDS提前关闭,在更大规模的研究中对整个干预措施进行评估之前需要进一步评估,评估可基于与患者相关的结果以及对临终护理的影响。
Clinicaltrials.gov(NCT02050256),2014年1月30日。