Australian and New Zealand Intensive Care Research Centre (ANZIC-RC), School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia.
National Trauma Research Institute, The Alfred, Monash University, Melbourne, Victoria, Australia.
PLoS One. 2018 Jun 21;13(6):e0198676. doi: 10.1371/journal.pone.0198676. eCollection 2018.
To appraise the currency, completeness and quality of evidence from systematic reviews (SRs) of acute management of moderate to severe traumatic brain injury (TBI).
We conducted comprehensive searches to March 2016 for published, English-language SRs and RCTs of acute management of moderate to severe TBI. Systematic reviews and RCTs were grouped under 12 broad intervention categories. For each review, we mapped the included and non-included RCTs, noting the reasons why RCTs were omitted. An SR was judged as 'current' when it included the most recently published RCT we found on their topic, and 'complete' when it included every RCT we found that met its inclusion criteria, taking account of when the review was conducted. Quality was assessed using the AMSTAR checklist (trichotomised into low, moderate and high quality).
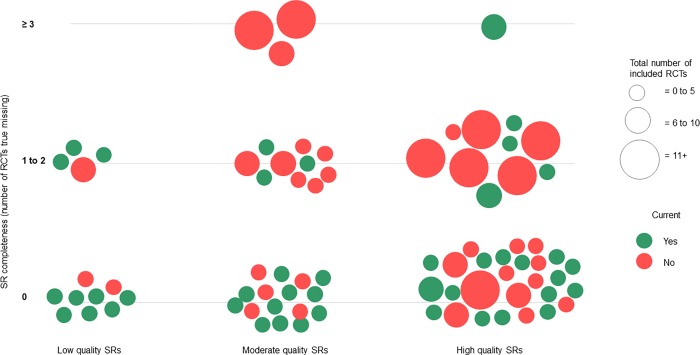
We included 85 SRs and 213 RCTs examining the effectiveness of treatments for acute management of moderate to severe TBI. The most frequently reviewed interventions were hypothermia (n = 17, 14.2%), hypertonic saline and/or mannitol (n = 9, 7.5%) and surgery (n = 8, 6.7%). Of the 80 single-intervention SRs, approximately half (n = 44, 55%) were judged as current and two-thirds (n = 52, 65.0%) as complete. When considering only the most recently published review on each intervention (n = 25), currency increased to 72.0% (n = 18). Less than half of the 85 SRs were judged as high quality (n = 38, 44.7%), and nearly 20% were low quality (n = 16, 18.8%). Only 16 (20.0%) of the single-intervention reviews (and none of the five multi-intervention reviews) were judged as current, complete and high-quality. These included reviews of red blood cell transfusion, hypothermia, management guided by intracranial pressure, pharmacological agents (various) and prehospital intubation. Over three-quarters (n = 167, 78.4%) of the 213 RCTs were included in one or more SR. Of the remainder, 17 (8.0%) RCTs post-dated or were out of scope of existing SRs, and 29 (13.6%) were on interventions that have not been assessed in SRs.
A substantial number of SRs in acute management of moderate to severe TBI lack currency, completeness and quality. We have identified both potential evidence gaps and also substantial research waste. Novel review methods, such as Living Systematic Reviews, may ameliorate these shortcomings and enhance utility and reliability of the evidence underpinning clinical care.
评价中度至重度创伤性脑损伤(TBI)急性治疗系统评价(SR)的货币价值、完整性和证据质量。
我们对 2016 年 3 月前发表的英语 SR 和中度至重度 TBI 急性治疗的 RCT 进行了全面检索。系统评价和 RCT 被分为 12 个广泛的干预类别。对于每一项研究,我们都绘制了纳入和未纳入的 RCT 图谱,记录了为什么排除了 RCT。当一项 SR 包括我们在其主题上发现的最新 RCT 时,该 SR 被认为是“最新的”,当它包括我们发现的每一项符合其纳入标准的 RCT 时,该 SR 被认为是“完整的”,同时考虑到进行 SR 的时间。使用 AMSTAR 清单(分为低、中、高质量)评估质量。
我们纳入了 85 项 SR 和 213 项 RCT,评估了治疗中度至重度 TBI 急性治疗的有效性。研究最频繁的干预措施是低温(n = 17,14.2%)、高渗盐水和/或甘露醇(n = 9,7.5%)和手术(n = 8,6.7%)。在 80 项单一干预措施的 SR 中,约有一半(n = 44,55%)被认为是最新的,三分之二(n = 52,65.0%)是完整的。当只考虑每一种干预措施中最新发表的综述(n = 25)时,最新率增加到 72.0%(n = 18)。85 项 SR 中不到一半(n = 38,44.7%)被认为是高质量的,近 20%(n = 16,18.8%)是低质量的。只有 16 项(20.0%)的单一干预措施综述(没有一项是五项多干预措施综述)被认为是最新的、完整的和高质量的。这些综述包括红细胞输注、低温、颅内压指导的管理、药物治疗(各种)和院前插管的综述。213 项 RCT 中有超过四分之三(n = 167,78.4%)被纳入了一项或多项 SR。其余的 17 项(8.0%)RCT 日期较晚或超出了现有 SR 的范围,29 项(13.6%)涉及的干预措施尚未在 SR 中评估。
中度至重度 TBI 急性治疗的大量 SR 缺乏及时性、完整性和质量。我们已经确定了潜在的证据差距,也存在大量的研究浪费。新的综述方法,如活体系统综述,可能会改善这些缺点,并提高临床护理证据的实用性和可靠性。