Hewner Sharon, Casucci Sabrina, Sullivan Suzanne, Mistretta Francine, Xue Yuqing, Johnson Barbara, Pratt Rebekah, Lin Li, Fox Chester
University at Buffalo.
Elmwood Health Center.
EGEMS (Wash DC). 2017 Jul 4;5(2):2. doi: 10.13063/2327-9214.1282.
Care continuity during transitions between the hospital and home requires reliable communication between providers and settings and an understanding of social determinants that influence recovery.
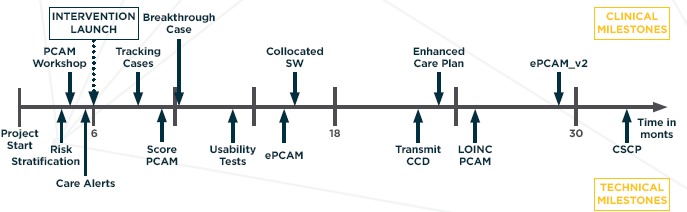
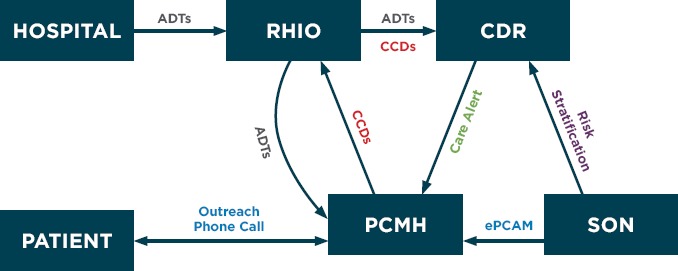
The coordinating transitions intervention uses real time alerts, delivered directly to the primary care practice for complex chronically ill patients discharged from an acute care setting, to facilitate nurse care coordinator led telephone outreach. The intervention incorporates claims-based risk stratification to prioritize patients for follow-up and an assessment of social determinants of health using the Patient-centered Assessment Method (PCAM). Results from transitional care are stored and transmitted to qualified healthcare providers across the continuum.
Reliance on tools that incorporated interoperability standards facilitated exchange of health information between the hospital and primary care. The PCAM was incorporated into both the clinical and informational workflow through the collaboration of clinical, industry, and academic partners. Health outcomes improved at the study practice over their baseline and in comparison with control practices and the regional Medicaid population.
Current research supports the potential impact of systems approaches to care coordination in improving utilization value after discharge. The project demonstrated that flexibility in developing the informational and clinical workflow was critical in developing a solution that improved continuity during transitions. There is additional work needed in developing managerial continuity across settings such as shared comprehensive care plans.
New clinical and informational workflows which incorporate social determinant of health data into standard practice transformed clinical practice and improved outcomes for patients.
医院和家庭之间过渡期间的护理连续性需要提供者与不同环境之间进行可靠的沟通,以及对影响康复的社会决定因素的理解。
协调过渡干预措施使用实时警报,直接发送到初级保健机构,用于从急性护理机构出院的复杂慢性病患者,以促进由护士护理协调员主导的电话随访。该干预措施采用基于索赔的风险分层来确定随访患者的优先级,并使用以患者为中心的评估方法(PCAM)对健康的社会决定因素进行评估。过渡护理的结果被存储并传输给整个连续过程中的合格医疗保健提供者。
对采用互操作性标准的工具的依赖促进了医院和初级保健机构之间的健康信息交换。通过临床、行业和学术伙伴的合作,PCAM被纳入临床和信息工作流程。与基线相比,以及与对照机构和地区医疗补助人群相比,研究机构的健康结果得到改善。
当前研究支持护理协调系统方法在提高出院后利用价值方面的潜在影响。该项目表明,在开发信息和临床工作流程时保持灵活性对于开发一种改善过渡期间连续性的解决方案至关重要。在跨不同环境(如共享综合护理计划)发展管理连续性方面还需要开展更多工作。
将健康数据的社会决定因素纳入标准实践的新临床和信息工作流程改变了临床实践并改善了患者的结局。