Choi Seung Jun, Moon Sena, Choi Ui Yoon, Chun Yoon Hong, Lee Jung Hyun, Rhim Jung Woo, Lee Jin, Kim Hwang Min, Jeong Dae Chul
Department of Pediatrics, Asan Medical Center Children's Hospital, University of Ulsan College of Medicine, Seoul, Republic of Korea.
Graduate School of Medicine, The Catholic University of Korea, College of Medicine, Seoul, Republic of Korea.
BMC Pediatr. 2018 Jun 23;18(1):201. doi: 10.1186/s12887-018-1166-z.
We aimed to compare the antipyretic efficacy, safety, and tolerability between oral dexibuprofen and intravenous propacetamol in children with upper respiratory tract infection (URTI) presenting with fever.
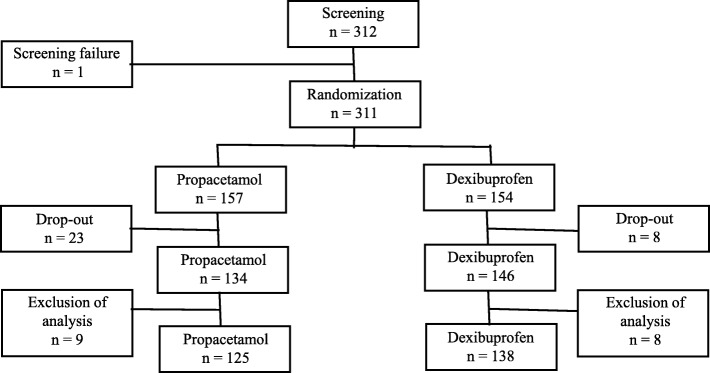
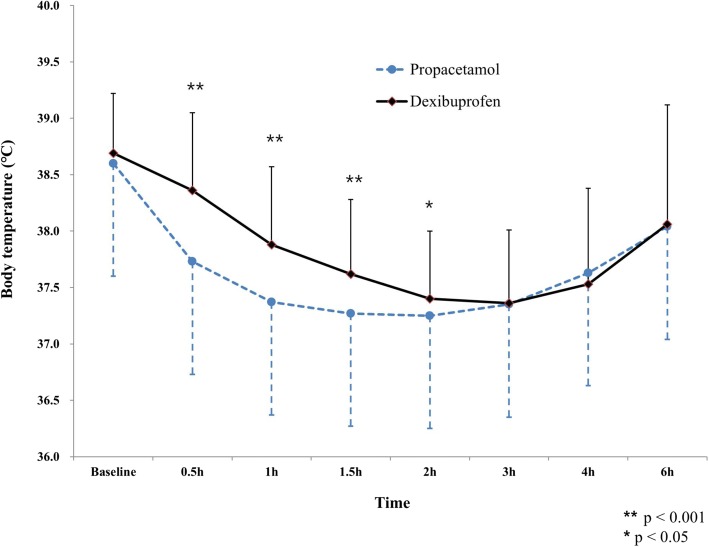
Patients aging from 6 months to 14 years admitted for URTI with axillary body temperature ≥ 38.0 °C were enrolled and randomized into the study or control group. Patients in the study group were intravenously infused with propacetamol and subsequently oral placebo medication was administered. Patients in the control group were intravenously infused with 100 mL of 0.9% sodium chloride solution without propacetamol and then oral dexibuprofen was administered. We checked the body temperature of all patients at 0.5 h (hr), 1 h, 1.5 h, 2 h, 3 h, 4 h, and 6 h after oral placebo or dexibuprofen had been applied.
A total of 263 patients (125 in the study group) were finally enrolled. The body temperatures of patients in the study group were significantly lower until 2 h after administration (37.73 ± 0.58 vs 38.36 ± 0.69 °C (p < 0.001), 37.37 ± 0.53 vs 37.88 ± 0.69 °C (p < 0.001), 37.27 ± 0.60 vs 37.62 ± 0.66 °C (p < 0.001), 37.25 ± 0.62 vs 37.40 ± 0.60 °C (p = 0.0452), at 0.5 h, 1 h, 1.5 h, and 2 h, respectively). The two groups showed no significant differences in terms of the range of body temperature decrease, the Area Under the Curve of body temperature change for antipyretic administration-and-time relationship, the maximum value of body temperature decrease during the 6 h test period, the number of patients whose body temperature normalized (< 37.0 °C), the mean time when first normalization of body temperature, and the development of adverse events including gastrointestinal problem, elevated liver enzyme, and thrombocytopenia.
Intravenous propacetamol may be a safe and effective choice for pediatric URTI patients presenting with fever who are not able to take oral medications or need faster fever control.
CRIS KCT0002888 . Date of registration: July 31st, 2013.
我们旨在比较口服右布洛芬与静脉注射丙帕他莫对患有上呼吸道感染(URTI)并发热儿童的退热疗效、安全性和耐受性。
纳入年龄在6个月至14岁、因URTI入院且腋窝体温≥38.0°C的患者,并随机分为研究组或对照组。研究组患者静脉输注丙帕他莫,随后给予口服安慰剂。对照组患者静脉输注100mL不含丙帕他莫的0.9%氯化钠溶液,然后口服右布洛芬。在口服安慰剂或右布洛芬后0.5小时(h)、1小时、1.5小时、2小时、3小时、4小时和6小时检查所有患者的体温。
最终共纳入263例患者(研究组125例)。研究组患者在给药后2小时内体温显著较低(分别在0.5小时、1小时、1.5小时和2小时时,体温为37.73±0.58 vs 38.36±0.69°C(p<0.001),37.37±0.53 vs 37.88±0.69°C(p<0.001),37.27±0.60 vs 37.62±0.66°C(p<0.001),37.25±0.62 vs 37.40±0.60°C(p = 0.0452))。两组在体温下降幅度、退热给药与时间关系的体温变化曲线下面积、6小时测试期内体温下降的最大值、体温恢复正常(<37.0°C)的患者数量、首次体温恢复正常的平均时间以及包括胃肠道问题、肝酶升高和血小板减少在内的不良事件发生情况方面均无显著差异。
对于不能口服药物或需要更快控制发热的小儿URTI发热患者,静脉注射丙帕他莫可能是一种安全有效的选择。
CRIS KCT0002888。注册日期:2013年7月31日。