Duke Clinical Research Institute, Duke University School of Medicine, Durham, NC
Duke Clinical Research Institute, Duke University School of Medicine, Durham, NC.
J Am Heart Assoc. 2018 Jun 30;7(13):e007230. doi: 10.1161/JAHA.117.007230.
There is limited information about the long-term survival of older patients after myocardial infarction (MI).
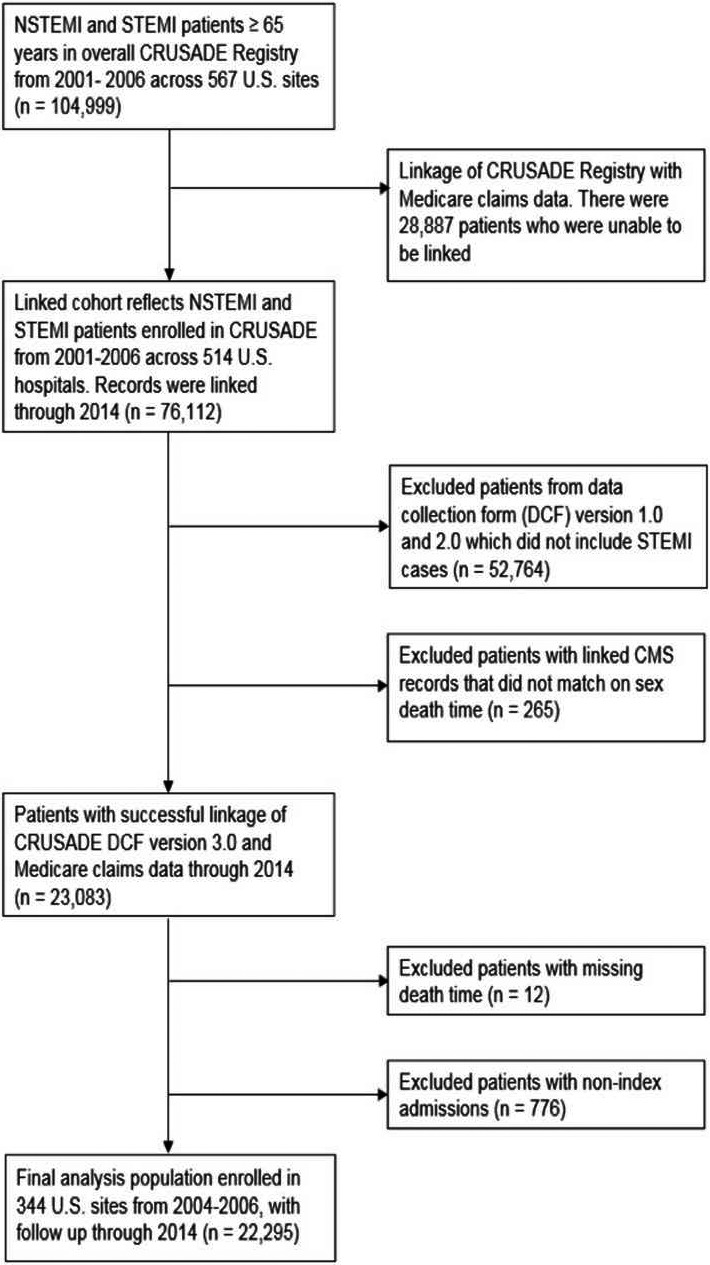
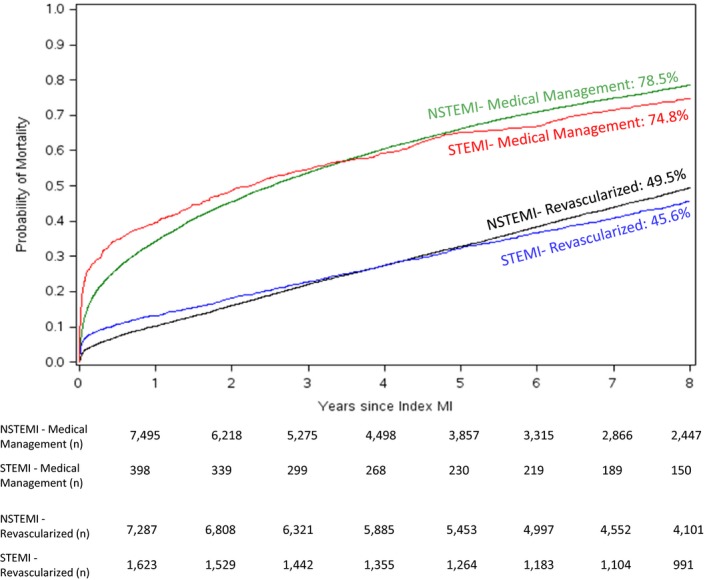
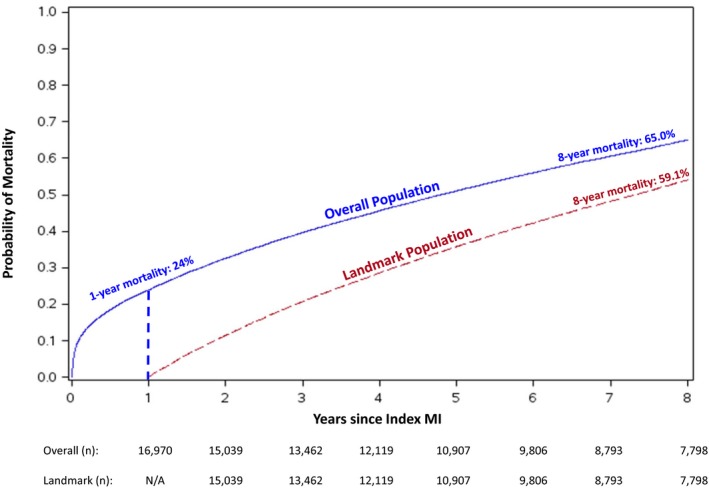
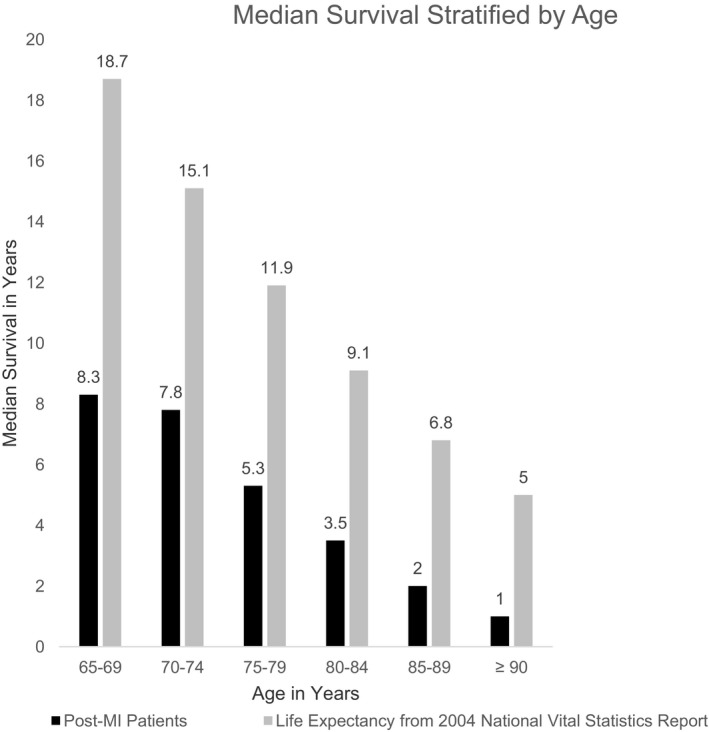
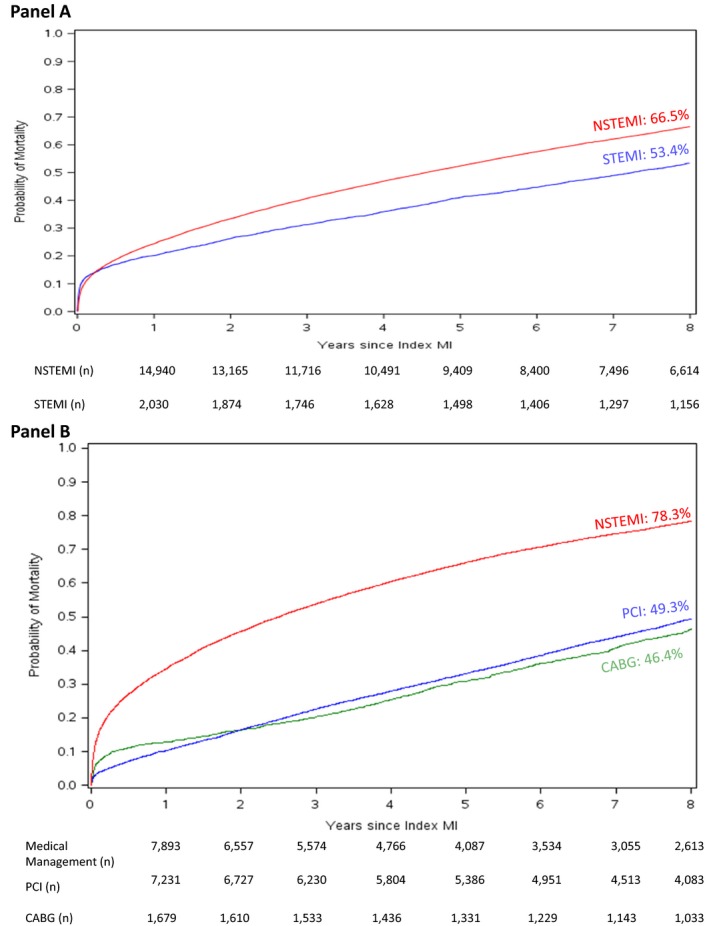
CRUSADE (Can rapid risk stratification of unstable angina patients suppress adverse outcomes with early implementation of the ACC/AHA guidelines) was a registry of MI patients treated at 568 US hospitals from 2001 to 2006. We linked MI patients aged ≥65 years in CRUSADE to their Medicare data to ascertain long-term mortality (defined as 8 years post index event). Long-term unadjusted Kaplan-Meier mortality curves were examined among patients stratified by revascularization status. A landmark analysis conditioned on surviving the first year post-MI was conducted. We used multivariable Cox regression to compare mortality risks between ST-segment-elevation myocardial infarction and non-ST-segment-elevation myocardial infarction patients. Among 22 295 MI patients ≥ age 65 years (median age 77 years), we observed high rates of evidence-based medication use at discharge: aspirin 95%, β-blockers 94%, and statins 81%. Despite this, mortality rates were high: 24% at 1 year, 51% at 5 years, and 65% at 8 years. Eight-year mortality remained high among patients who underwent percutaneous coronary intervention (49%), coronary artery bypass graft (46%), and among patients who survived the first year post-MI (59%). Median survival was 4.8 years (25th, 75th percentiles 1.1, 8.5); among patients aged 65-74 years it was 8.2 years (3.3, 8.9) while for patients aged ≥75 years it was 3.1 years (0.6, 7.6). Eight-year mortality was lower among ST-segment-elevation myocardial infarction than non-ST-segment-elevation myocardial infarction patients (53% versus 67%); this difference was not significant after adjustment (hazard ratio 0.94, 95% confidence interval, 0.88-1.00).
Long-term mortality remains high among patients with MI in routine clinical practice, even among revascularized patients and those who survived the first year.
关于心肌梗死(MI)后老年患者的长期生存情况,相关信息有限。
CRUSADE(不稳定型心绞痛患者快速危险分层能否通过早期实施 ACC/AHA 指南来降低不良结局)是一项 2001 年至 2006 年在美国 568 家医院治疗的 MI 患者注册研究。我们将 CRUSADE 中年龄≥65 岁的 MI 患者与他们的医疗保险数据相联系,以确定长期死亡率(定义为索引事件后 8 年)。根据血管重建状态对患者进行分层,检查长期未经调整的 Kaplan-Meier 死亡率曲线。对 MI 后存活满 1 年的患者进行了一个基于时间的分析。我们使用多变量 Cox 回归比较 ST 段抬高型心肌梗死和非 ST 段抬高型心肌梗死患者的死亡率风险。在 22295 名年龄≥65 岁的 MI 患者(中位年龄 77 岁)中,我们观察到出院时使用循证药物的比例很高:阿司匹林 95%、β受体阻滞剂 94%和他汀类药物 81%。尽管如此,死亡率仍然很高:1 年时为 24%,5 年时为 51%,8 年时为 65%。接受经皮冠状动脉介入治疗(49%)、冠状动脉旁路移植术(46%)和 MI 后存活满 1 年的患者(59%)8 年死亡率仍然很高。中位生存时间为 4.8 年(25%,75%分位数 1.1,8.5);年龄在 65-74 岁的患者为 8.2 年(3.3,8.9),而年龄≥75 岁的患者为 3.1 年(0.6,7.6)。ST 段抬高型心肌梗死患者的 8 年死亡率低于非 ST 段抬高型心肌梗死患者(53%比 67%);但调整后差异无统计学意义(风险比 0.94,95%置信区间,0.88-1.00)。
即使在血管重建患者和 MI 后存活满 1 年的患者中,常规临床实践中 MI 患者的长期死亡率仍然很高。