Choo Eun Ho, Han Eun Ji, Kim Chan Joon, Kim Sung Hoon, O Joo Hyun, Chang Kiyuk, Seung Ki Bae
Department of Cardiology, The Catholic University of Korea College of Medicine, Seoul, Korea.
Department of Radiology, The Catholic University of Korea College of Medicine, Seoul, Korea.
Korean Circ J. 2018 Jul;48(7):591-601. doi: 10.4070/kcj.2017.0029.
Non-statin therapy plus lower intensity statin might be an alternative in patients with coronary artery disease (CAD). A recent data suggested an anti-inflammatory therapy can reduce recurrent cardiovascular events and pioglitazone is also an intriguing inflammatory-modulating agent. However, limited data exist on whether pioglitazone on top of statins further attenuates plaque inflammation.
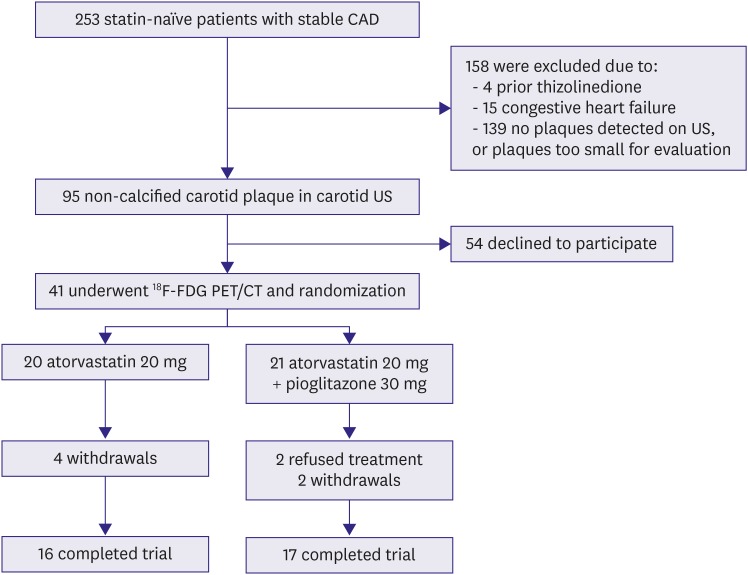
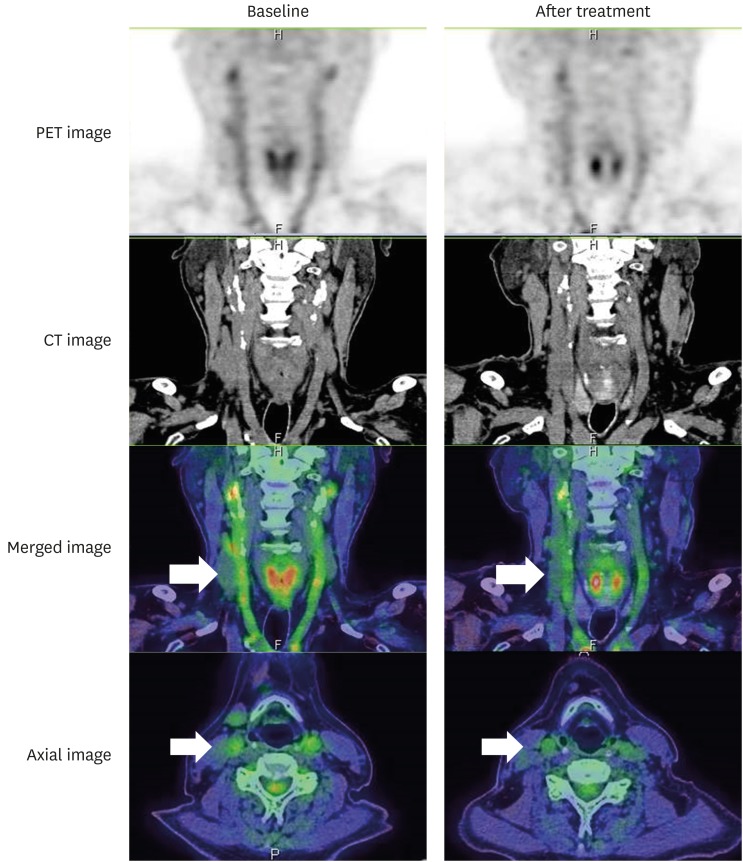
Statin-naïve patients with stable CAD and carotid plaques of ≥3 mm were randomly prescribed moderate dose atorvastatin (20 mg/day), or moderate dose atorvastatin plus pioglitazone (30 mg/day) for 3 months. The primary endpoint was the change in the arterial inflammation of the carotid artery measured by ¹⁸F-fluorodeoxyglucose positron emission tomography/computed tomography (¹⁸F-FDG-PET/CT) during 3 months.
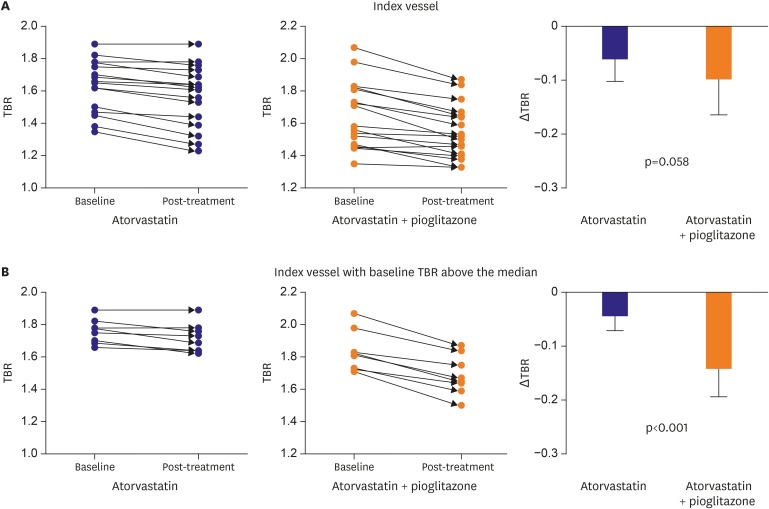
Of the 41 randomized patients, 33 underwent an evaluation by fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT; 17 atorvastatin plus pioglitazone and 16 atorvastatin patients). The addition of pioglitazone significantly improved the insulin sensitivity and increased the high-density lipoprotein cholesterol after 3 months. Although a reduction in the (FDG) uptake by pioglitazone on top of atorvastatin in carotid arteries with plaque showed marginally statistical significance in the entire patient group (atorvastatin plus pioglitazone; -0.10±0.07 and atorvastatin -0.06±0.04, p=0.058), pioglitazone showed a further reduction of the fluorodeoxyglucose (FDG) uptake among patients who had a baseline FDG uptake above the median (atorvastatin plus pioglitazone; -0.14±0.04 and atorvastatin -0.03±0.03, p<0.001).
Pioglitazone demonstrated marginally significant anti-inflammatory effects in addition to moderate dose atorvastatin. This may have been due to the lack of power of the study. However, pioglitazone may have an anti-inflammatory effect in those patients with high plaque inflammation (Trial registry at ClinicalTrials.gov, NCT01341730).
对于冠状动脉疾病(CAD)患者,非他汀类疗法联合低强度他汀可能是一种替代方案。最近的数据表明,抗炎疗法可减少心血管事件复发,而吡格列酮也是一种引人关注的炎症调节药物。然而,关于在他汀类药物基础上加用吡格列酮是否能进一步减轻斑块炎症的数据有限。
将初治的稳定型CAD且颈动脉斑块≥3mm的患者随机分为两组,分别给予中等剂量阿托伐他汀(20mg/天)或中等剂量阿托伐他汀联合吡格列酮(30mg/天),治疗3个月。主要终点是通过¹⁸F-氟脱氧葡萄糖正电子发射断层扫描/计算机断层扫描(¹⁸F-FDG-PET/CT)测量的3个月内颈动脉动脉炎症的变化。
41例随机分组的患者中,33例接受了氟脱氧葡萄糖正电子发射断层扫描/计算机断层扫描(FDG-PET/CT)评估(17例接受阿托伐他汀联合吡格列酮治疗,16例接受阿托伐他汀治疗)。加用吡格列酮3个月后显著改善了胰岛素敏感性并提高了高密度脂蛋白胆固醇水平。虽然在整个患者组中,在有斑块的颈动脉中,吡格列酮联合阿托伐他汀使(FDG)摄取降低在统计学上仅具有边缘显著性(阿托伐他汀联合吡格列酮组为-0.10±0.07,阿托伐他汀组为-0.06±0.04,p=0.058),但在基线FDG摄取高于中位数的患者中,吡格列酮使氟脱氧葡萄糖(FDG)摄取进一步降低(阿托伐他汀联合吡格列酮组为-0.14±0.04,阿托伐他汀组为-0.03±0.03,p<0.001)。
除中等剂量阿托伐他汀外,吡格列酮显示出边缘显著的抗炎作用。这可能是由于该研究的效能不足。然而,吡格列酮可能对那些斑块炎症程度高的患者具有抗炎作用(临床试验注册于ClinicalTrials.gov,NCT01341730)。