Guo Zhen-Ni, Sun Xin, Liu Jia, Sun Huijie, Zhao Yingkai, Ma Hongyin, Xu Baofeng, Wang Zhongxiu, Li Chao, Yan Xiuli, Zhou Hongwei, Zhang Peng, Jin Hang, Yang Yi
Department of Neurology, The First Hospital of Jilin University, Changchun, China.
Department of Neurology, Clinical Trial and Research Center for Stroke, The First Hospital of Jilin University, Changchun, China.
Front Physiol. 2018 Jun 19;9:759. doi: 10.3389/fphys.2018.00759. eCollection 2018.
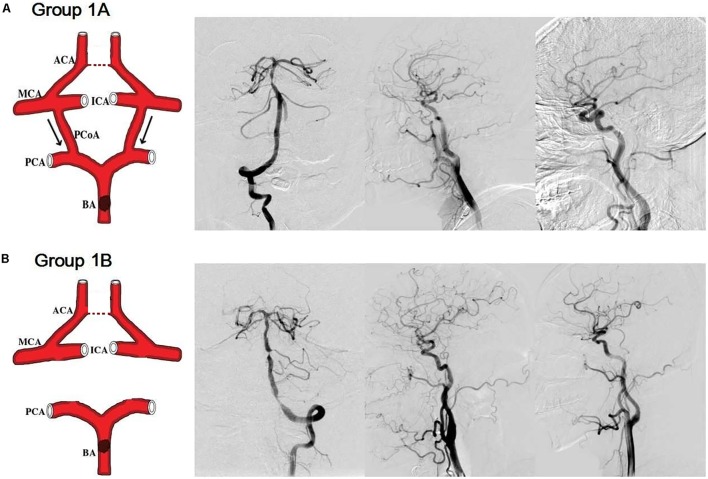
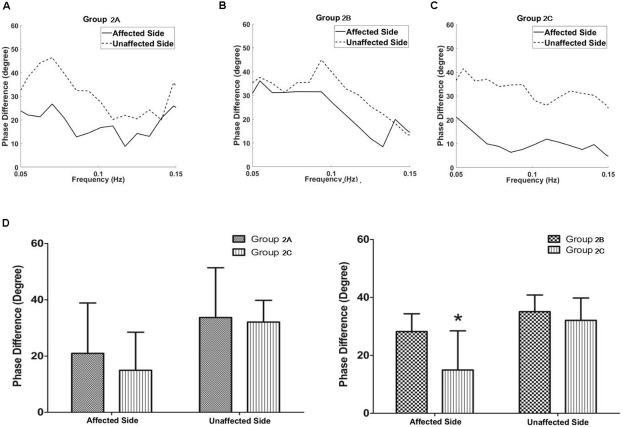
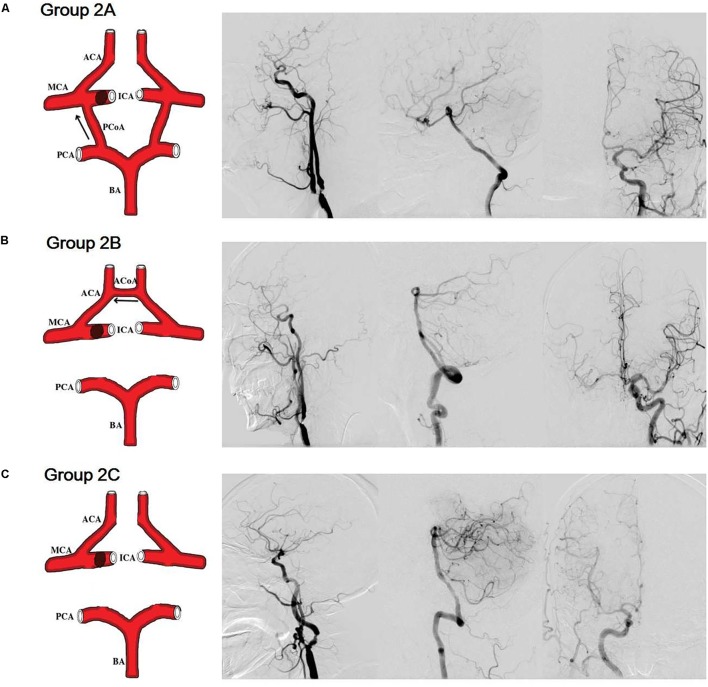
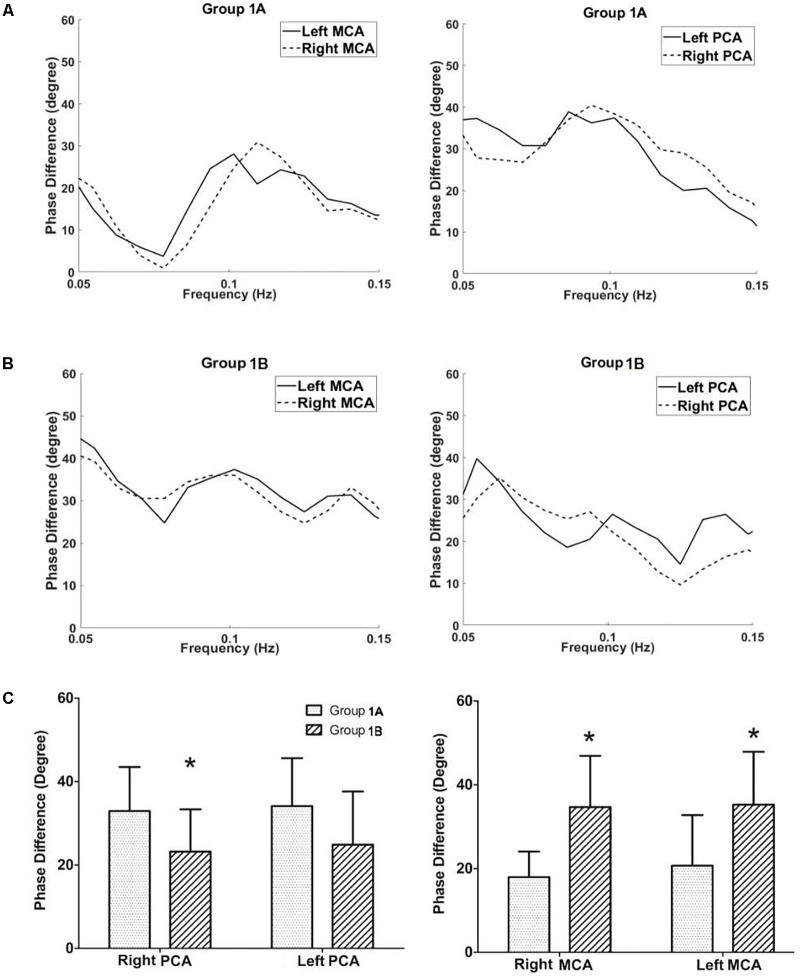
The influence of the anterior and posterior communicating artery (ACoA and PCoA) on dynamic cerebral autoregulation (dCA) is largely unknown. In this study, we aimed to test whether substantial differences in collateral anatomy were associated with differences in dCA in two common types of stenosis according to digital subtraction angiography (DSA): either isolated basal artery and/or bilateral vertebral arteries severe stenosis/occlusion (group 1; group 1A: with bilateral PCoAs; and group 1B: without bilateral PCoAs), or isolated unilateral internal carotid artery severe stenosis/occlusion (group 2; group 2A: without ACoA and with PCoA; group 2B: with ACoA and without PCoAs; and group 2C: without both ACoA and PCoA). The dCA was calculated by transfer function analysis (a mathematical model), and was evaluated in middle cerebral artery (MCA) and/or posterior cerebral artery (PCA). Of a total of 231 non-acute phase ischemic stroke patients who received both dCA assessment and DSA in our lab between 2014 and 2017, 51 patients met inclusion criteria based on the presence or absence of ACoA or PCoA, including 21 patients in the group 1, and 30 patients in the group 2. There were no significant differences in gender, age, and mean blood pressure between group 1A and group 1B, and among group 2A, group 2B, and group 2C. In group 1, the PCA phase difference values (autoregulatory parameter) were significantly higher in the subgroup with patent PCoAs, compared to those without. In group 2, the MCA phase difference values were higher in the subgroup with patent ACoA, compared to those without. This pilot study found that the cross-flow of the ACoA/PCoA to the affected area compensates for compromised dCA in the affected area, which suggests an important role of the ACoA/PCoA in stabilizing cerebral blood flow.
前交通动脉和后交通动脉(ACoA和PCoA)对动态脑自动调节(dCA)的影响在很大程度上尚不清楚。在本研究中,我们旨在根据数字减影血管造影(DSA),测试在两种常见类型的狭窄中,侧支循环解剖结构的显著差异是否与dCA的差异相关:即孤立的基底动脉和/或双侧椎动脉严重狭窄/闭塞(第1组;第1A组:有双侧PCoA;第1B组:无双侧PCoA),或孤立的单侧颈内动脉严重狭窄/闭塞(第2组;第2A组:无ACoA且有PCoA;第2B组:有ACoA且无PCoA;第2C组:无ACoA和PCoA)。dCA通过传递函数分析(一种数学模型)计算得出,并在大脑中动脉(MCA)和/或大脑后动脉(PCA)中进行评估。在20XX年至20XX年期间,我们实验室共有231例接受dCA评估和DSA的非急性期缺血性中风患者,其中51例根据ACoA或PCoA的有无符合纳入标准,包括第1组中的21例患者和第2组中的30例患者。第1A组和第1B组之间,以及第2A组、第2B组和第2C组之间在性别、年龄和平均血压方面无显著差异。在第1组中,与无PCoA的亚组相比,有PCoA的亚组中PCA相位差值(自动调节参数)显著更高。在第2组中,与无ACoA的亚组相比,有ACoA的亚组中MCA相位差值更高。这项初步研究发现,ACoA/PCoA向受影响区域的交叉血流可补偿受影响区域受损的dCA,这表明ACoA/PCoA在稳定脑血流量方面具有重要作用。