Division of Primary Care, 13th floor, Tower Building, University Park, University of Nottingham, Nottingham NG2 7RD, UK
Division of Primary Care, 13th floor, Tower Building, University Park, University of Nottingham, Nottingham NG2 7RD, UK.
BMJ. 2018 Jul 4;362:k2505. doi: 10.1136/bmj.k2505.
To investigate the associations between direct oral anticoagulants (DOACs) and risks of bleeding, ischaemic stroke, venous thromboembolism, and all cause mortality compared with warfarin.
Prospective open cohort study.
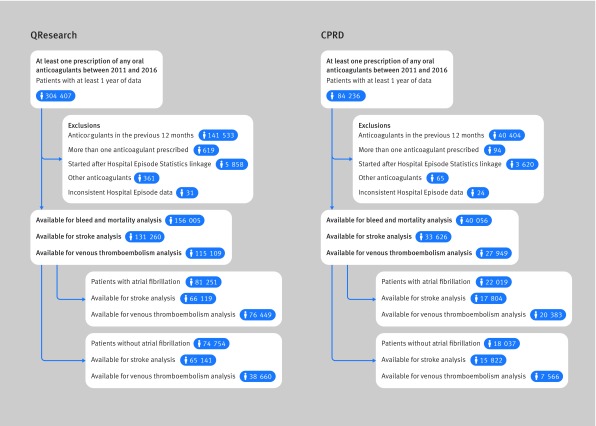
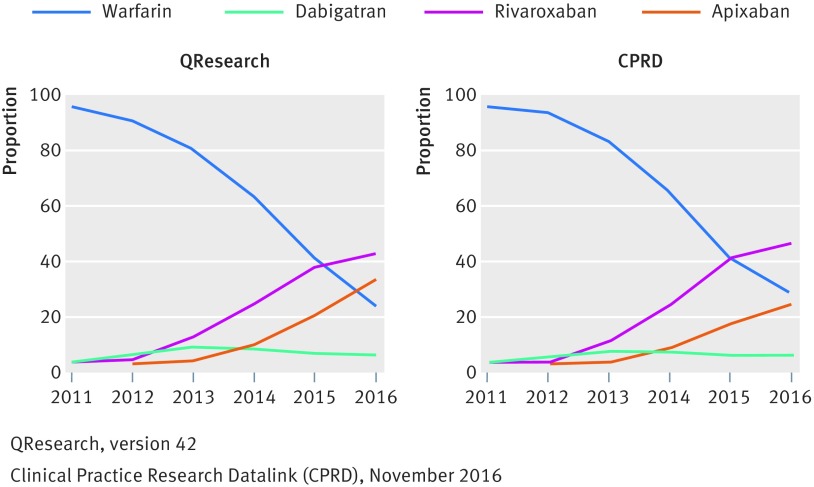
UK general practices contributing to QResearch or Clinical Practice Research Datalink.
132 231 warfarin, 7744 dabigatran, 37 863 rivaroxaban, and 18 223 apixaban users without anticoagulant prescriptions for 12 months before study entry, subgrouped into 103 270 patients with atrial fibrillation and 92 791 without atrial fibrillation between 2011 and 2016.
Major bleeding leading to hospital admission or death. Specific sites of bleeding and all cause mortality were also studied.
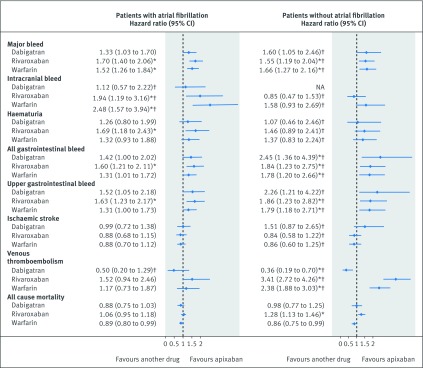
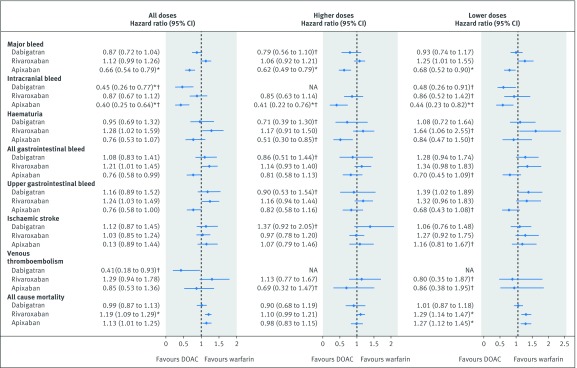
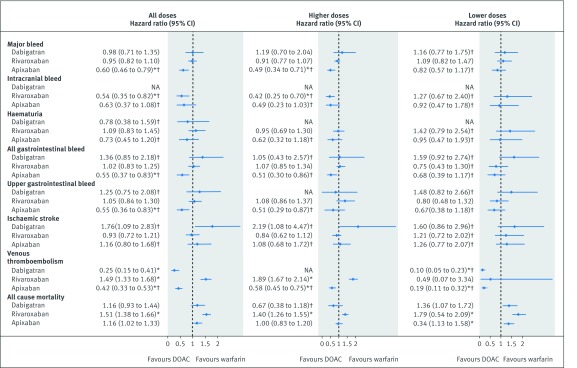
In patients with atrial fibrillation, compared with warfarin, apixaban was associated with a decreased risk of major bleeding (adjusted hazard ratio 0.66, 95% confidence interval 0.54 to 0.79) and intracranial bleeding (0.40, 0.25 to 0.64); dabigatran was associated with a decreased risk of intracranial bleeding (0.45, 0.26 to 0.77). An increased risk of all cause mortality was observed in patients taking rivaroxaban (1.19, 1.09 to 1.29) or on lower doses of apixaban (1.27, 1.12 to 1.45). In patients without atrial fibrillation, compared with warfarin, apixaban was associated with a decreased risk of major bleeding (0.60, 0.46 to 0.79), any gastrointestinal bleeding (0.55, 0.37 to 0.83), and upper gastrointestinal bleeding (0.55, 0.36 to 0.83); rivaroxaban was associated with a decreased risk of intracranial bleeding (0.54, 0.35 to 0.82). Increased risk of all cause mortality was observed in patients taking rivaroxaban (1.51, 1.38 to 1.66) and those on lower doses of apixaban (1.34, 1.13 to 1.58).
Overall, apixaban was found to be the safest drug, with reduced risks of major, intracranial, and gastrointestinal bleeding compared with warfarin. Rivaroxaban and low dose apixaban were, however, associated with increased risks of all cause mortality compared with warfarin.
与华法林相比,评估直接口服抗凝剂(DOACs)与出血、缺血性卒、静脉血栓栓塞和全因死亡率风险之间的关联。
前瞻性开放队列研究。
参与 QResearch 或临床实践研究数据链接的英国普通实践。
132231 名华法林、7744 名达比加群、37863 名利伐沙班和 18223 名阿哌沙班患者,在研究入组前的 12 个月内没有抗凝处方,分为 2011 年至 2016 年期间患有心房颤动的 103270 名和无心房颤动的 92791 名患者。
主要出血导致住院或死亡。还研究了特定部位出血和全因死亡率。
在患有心房颤动的患者中,与华法林相比,阿哌沙班与主要出血(校正风险比 0.66,95%置信区间 0.54 至 0.79)和颅内出血(0.40,0.25 至 0.64)风险降低相关;达比加群与颅内出血风险降低相关(0.45,0.26 至 0.77)。服用利伐沙班(1.19,1.09 至 1.29)或服用较低剂量阿哌沙班(1.27,1.12 至 1.45)的患者全因死亡率风险增加。在没有心房颤动的患者中,与华法林相比,阿哌沙班与主要出血(0.60,0.46 至 0.79)、任何胃肠道出血(0.55,0.37 至 0.83)和上胃肠道出血(0.55,0.36 至 0.83)风险降低相关;利伐沙班与颅内出血风险降低相关(0.54,0.35 至 0.82)。服用利伐沙班(1.51,1.38 至 1.66)和服用较低剂量阿哌沙班(1.34,1.13 至 1.58)的患者全因死亡率风险增加。
总体而言,与华法林相比,阿哌沙班是最安全的药物,主要出血、颅内出血和胃肠道出血的风险降低。然而,与华法林相比,利伐沙班和低剂量阿哌沙班与全因死亡率风险增加相关。