Luo Xin, Yang Xiang, Li Jiexian, Zou Ge, Lin Yufeng, Qing Guoqiang, Yang Ruilin, Yao Weixiang, Ye Xuying
Department of Urology Department of Gynecology, Panyu Central Hospital, Guangzhou, China.
Medicine (Baltimore). 2018 Jul;97(28):e11078. doi: 10.1097/MD.0000000000011078.
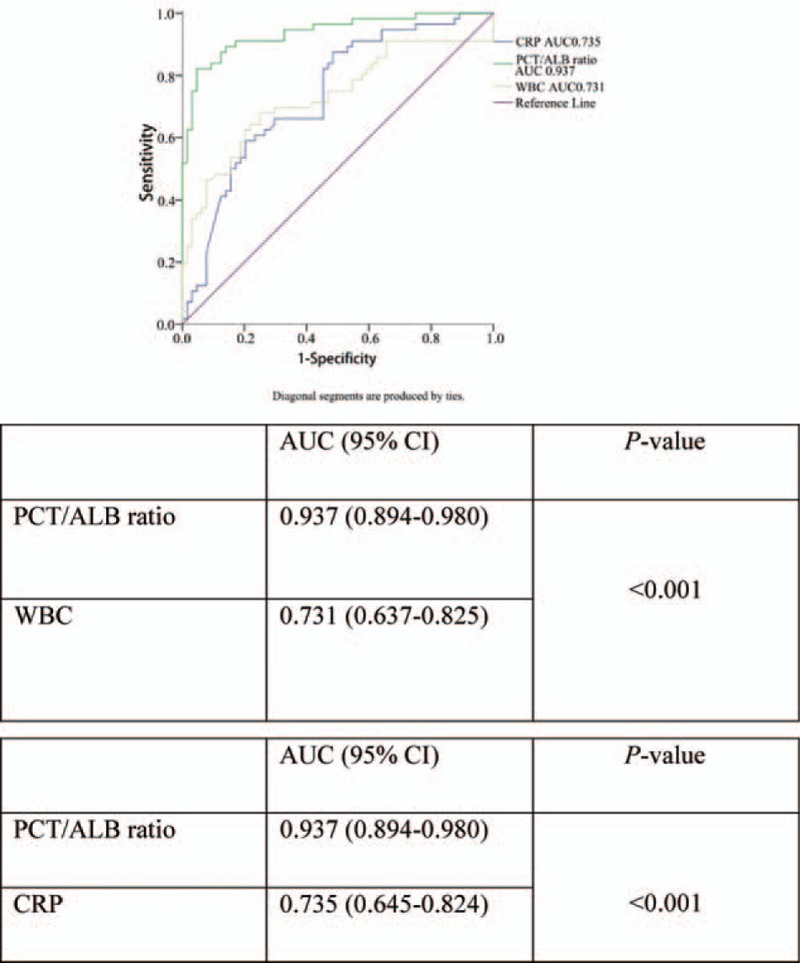
Discrimination between urosepsis and febrile urinary tract infections is important in therapeutic decision-making to indicate suitable treatments to avoid sepsis-related organ failure. Accurate diagnosis is time-consuming and susceptible to false-positive results. Moreover, patient responses to urosepsis are complex and varied. Therefore, this study aimed to develop a new, early diagnostic predictor that could discriminate between patients with urosepsis and those with febrile urinary tract infections using a combination of initial procalcitonin and albumin levels.We conducted a retrospective study involving 140 patients with febrile urinary tract infections from January 2013 to December 2017. Univariate and multivariate logistic analyses were performed to identify the independent risk factors for differentiating urosepsis from febrile urinary tract infection. A receiver operating characteristic (ROC) curve analysis was conducted to compare the predictive accuracy of the procalcitonin/albumin ratio.Patients in the urosepsis group had higher procalcitonin/albumin ratios compared to those in the febrile urinary tract infection group [2.254 (0.978, 6.299) vs 0.021 (0.004, 0.095); P < .001]. Based on multivariate logistic analysis, the procalcitonin/albumin ratio [adjusted odds ratio (OR) 1.029, 95% confidence interval (CI) 1.013-1.045, P < .001] was an independent predictor of urosepsis, which allowed for differentiation from patients with febrile urinary tract infections. The area under the ROC curve (AUC) for the procalcitonin/albumin ratio was 0.937 (95% CI, 0.894-0.980); P < .001. The sensitivity and specificity of the procalcitonin/albumin ratio cut-off values (>0.44) were 84.62% and 96.00%, respectively. Moreover, in the subset of 65 patients with urosepsis, the procalcitonin/albumin ratio in the uroseptic shock group was higher than in the group of patients without uroseptic shock [5.46 (1.43, 6.58) vs 1.24 (0.63, 4.38); P = .009].Our study demonstrates that the procalcitonin/albumin ratio is an early diagnostic predictor that can discriminate between urosepsis and febrile urinary tract infection. Additionally, in patients with urosepsis, those with higher procalcitonin/albumin ratios were more prone to uroseptic shock. Our findings suggest that the procalcitonin/albumin ratio is a rapid and relatively low-cost biomarker that can be used in clinical practice.
区分脓毒症和发热性尿路感染对于治疗决策很重要,有助于指明合适的治疗方法以避免与脓毒症相关的器官衰竭。准确诊断耗时且易出现假阳性结果。此外,患者对脓毒症的反应复杂多样。因此,本研究旨在开发一种新的早期诊断预测指标,该指标可通过联合使用初始降钙素原和白蛋白水平来区分脓毒症患者和发热性尿路感染患者。
我们进行了一项回顾性研究,纳入了2013年1月至2017年12月期间140例发热性尿路感染患者。进行单因素和多因素逻辑分析以确定区分脓毒症和发热性尿路感染的独立危险因素。进行受试者工作特征(ROC)曲线分析以比较降钙素原/白蛋白比值的预测准确性。
脓毒症组患者的降钙素原/白蛋白比值高于发热性尿路感染组[2.254(0.978,6.299)对0.021(0.004,0.095);P<0.001]。基于多因素逻辑分析,降钙素原/白蛋白比值[调整后的优势比(OR)1.029,95%置信区间(CI)1.013 - 1.045,P<0.001]是脓毒症的独立预测指标,可用于与发热性尿路感染患者进行区分。降钙素原/白蛋白比值的ROC曲线下面积(AUC)为0.937(95%CI,0.894 - 0.980);P<0.001。降钙素原/白蛋白比值临界值(>0.44)的敏感性和特异性分别为84.62%和96.00%。此外,在65例脓毒症患者亚组中,脓毒性休克组的降钙素原/白蛋白比值高于无脓毒性休克患者组[5.46(1.43,6.58)对1.24(0.63,4.38);P = 0.009]。
我们的研究表明,降钙素原/白蛋白比值是一种可区分脓毒症和发热性尿路感染的早期诊断预测指标。此外,在脓毒症患者中,降钙素原/白蛋白比值较高的患者更容易发生脓毒性休克。我们的研究结果表明,降钙素原/白蛋白比值是一种快速且成本相对较低的生物标志物,可用于临床实践。