Clinical Emergency County Hospital "Sf. Ap. Andrei", 800578 Galați, Romania.
Faculty of Medicine and Pharmacy, Dunarea de Jos University, 800008 Galați, Romania.
Medicina (Kaunas). 2023 Mar 17;59(3):597. doi: 10.3390/medicina59030597.
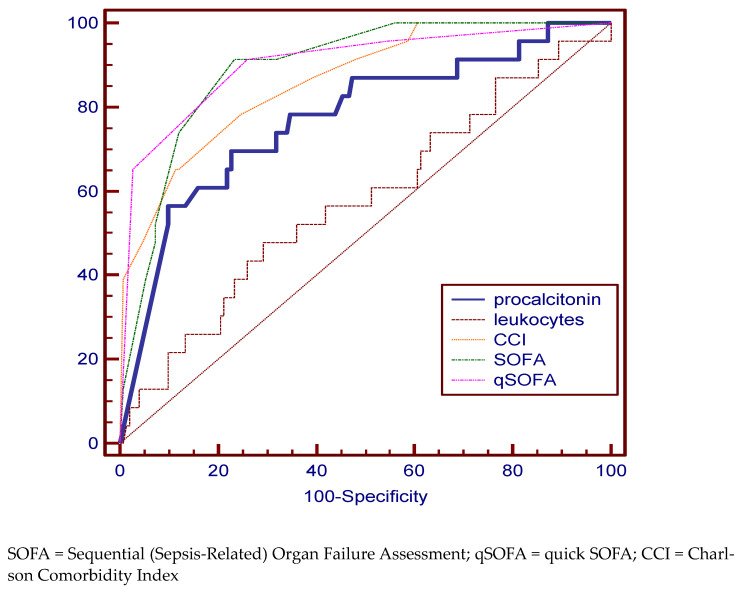
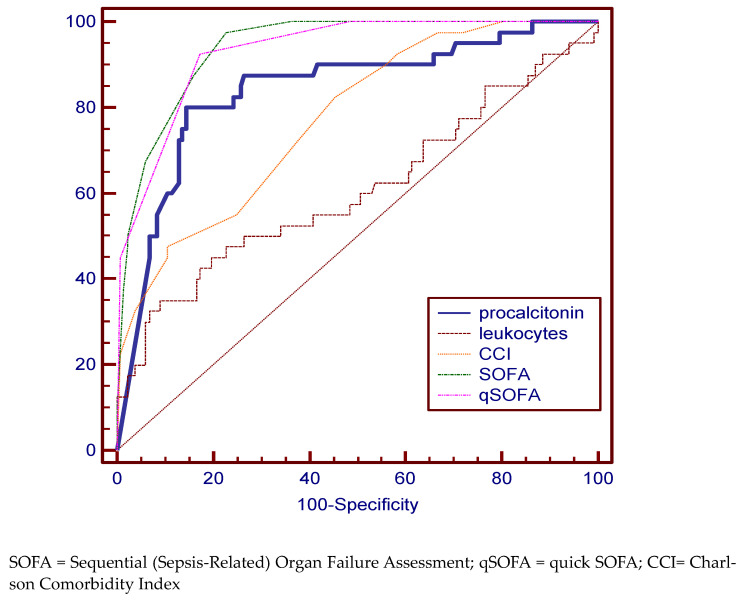
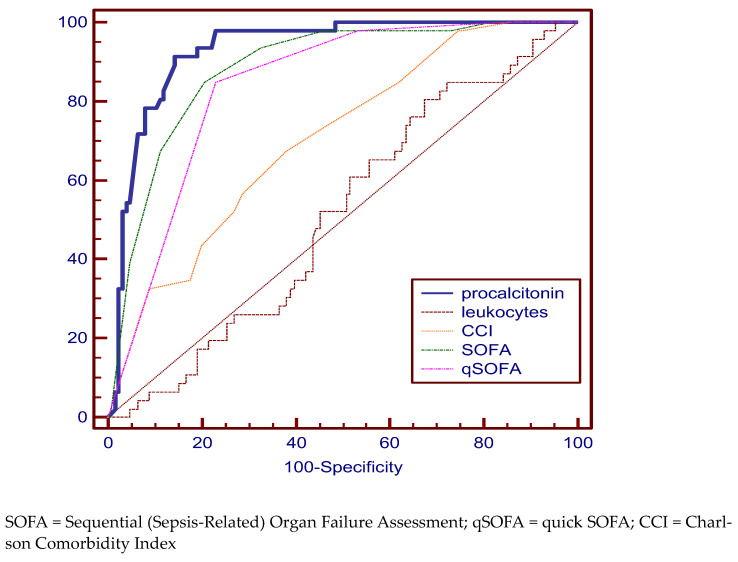
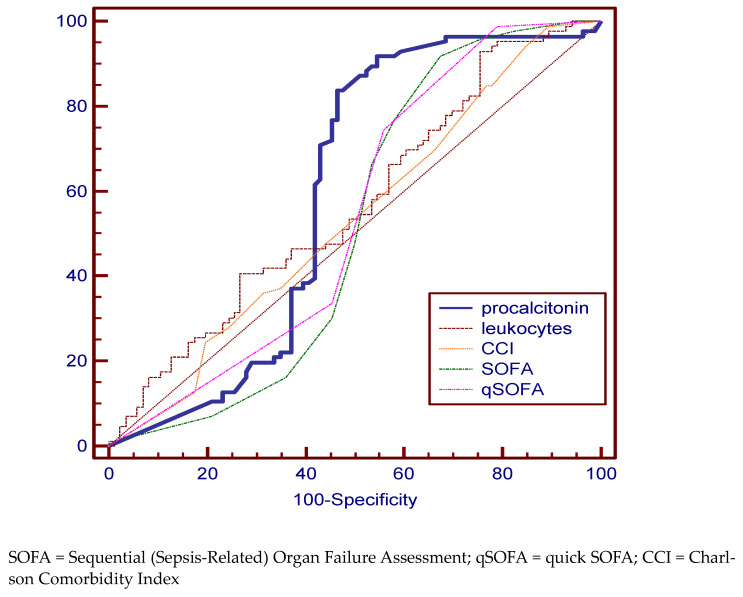
: Patients with urinary tract obstruction (UTO) and systemic inflammatory response syndrome (SIRS) are at risk of developing urosepsis, whose evolution involves increased morbidity, mortality and cost. The aim of this study is to evaluate the ability of already existing scores and biomarkers to diagnose, describe the clinical status, and predict the evolution of patients with complicated urinary tract infection (UTI) and their risk of progressing to urosepsis. : We conducted a retrospective study including patients diagnosed with UTI hospitalized in the urology department of" Sfântul Apostol Andrei" County Emergency Clinical Hospital (GCH) in Galati, Romania, from September 2019 to May 2022. The inclusion criteria were: UTI proven by urine culture or diagnosed clinically complicated with UTO, fever or shaking chills, and purulent collections, such as psoas abscess, Fournier Syndrome, renal abscess, and paraurethral abscess, showing SIRS. The exclusion criteria were: patients age < 18 years, pregnancy, history of kidney transplantation, hemodialysis or peritoneal dialysis, and patients with missing data. We used the Sequential (Sepsis-Related) Organ Failure Assessment (SOFA) and qSOFA (quick SOFA) scores, and procalcitonin (PCT) to describe the clinical status of the patients. The Charlson Comorbidity Index (CCI) was used to assesses pre-existing morbidities. The hospitalization days and costs and the days of intensive care were considered. Depending on the diagnosis at admission, we divided the patients into three groups: SIRS, sepsis and septic shock. The fourth group was represented by patients who died during hospitalization. : A total of 174 patients with complicated UTIs were enrolled in this study. From this total, 46 were enrolled in the SIRS group, 88 in the urosepsis group, and 40 in the septic shock group. A total of 23 patients died during hospitalization and were enrolled in the deceased group. An upward trend of age along with worsening symptoms was highlighted with an average of 56.86 years in the case of SIRS, 60.37 years in the sepsis group, 69.03 years in the septic shock, and 71.04 years in the case of deceased patients ( < 0.04). A statistically significant association between PCT and complex scores (SOFA, CCI and qSOFA) with the evolution of urosepsis was highlighted. Increased hospitalization costs can be observed in the case of deceased patients and those with septic shock and statistically significantly lower in the case of those with SIRS. The predictability of discriminating urosepsis stages was assessed by using the area under the ROC curve (AUC) and very good specificity and sensitivity was identified in predicting the risk of death for PCT (69.57%, 77.33%), the SOFA (91.33%, 76.82%), qSOFA (91.30%, 74.17%) scores, and CCI (65.22%, 88.74%). The AUC value was best for qSOFA (90.3%). For the SIRS group, the PCT (specificity 91.30%, sensitivity 85.71%) and SOFA (specificity 84.78%, sensitivity 78.74%), qSOFA scores (specificity 84.78%, sensitivity 76, 34%) proved to be relevant in establishing the diagnosis. In the case of the septic shock group, the qSOFA (specificity 92.5%, sensitivity 82.71%) and SOFA (specificity 97.5%, sensitivity 77.44%) as well as PCT (specificity 80%, sensitivity 85.61%) are statistically significant disease-defining variables. An important deficit in the tools needed to classify patients into the sepsis group is obvious. All the variables have an increased specificity but a low sensitivity. This translates into a risk of a false negative diagnosis. : Although SOFA and qSOFA scores adequately describe patients with septic shock and they are independent prognostic predictors of mortality, they fail to be accurate in diagnosing sepsis. These scores should not replace the conventional triage protocol. In our study, PCT proved to be a disease-defining marker and an independent prognostic predictor of mortality. Patients with important comorbidities, CCI greater than 10, should be treated more aggressively because of increased mortality.
: 患有尿路梗阻 (UTO) 和全身炎症反应综合征 (SIRS) 的患者有发生尿脓毒症的风险,其发展涉及更高的发病率、死亡率和成本。本研究旨在评估现有的评分和生物标志物在诊断、描述临床状况以及预测复杂尿路感染 (UTI) 患者的病情演变及其向尿脓毒症发展的风险方面的能力。 : 我们进行了一项回顾性研究,纳入了 2019 年 9 月至 2022 年 5 月在罗马尼亚加拉茨的“圣使徒安德鲁”县急症临床医院 (GCH) 泌尿科住院的 UTI 患者。纳入标准为:尿培养证实 UTI 或临床诊断为复杂 UTO,发热或寒战,有脓性积聚,如腰大肌脓肿、Fournier 综合征、肾脓肿和尿道旁脓肿,表现为 SIRS。排除标准为:年龄 < 18 岁、妊娠、肾移植、血液透析或腹膜透析史以及数据缺失的患者。我们使用序贯 (相关) 器官衰竭评估 (SOFA) 和快速 SOFA (qSOFA) 评分以及降钙素原 (PCT) 来描述患者的临床状况。 Charlson 合并症指数 (CCI) 用于评估预先存在的合并症。住院天数和费用以及重症监护天数都被考虑在内。根据入院时的诊断,我们将患者分为三组:SIRS、败血症和败血症性休克。第四组由住院期间死亡的患者组成。 : 共有 174 名复杂 UTI 患者纳入本研究。其中 46 例被纳入 SIRS 组,88 例被纳入尿脓毒症组,40 例被纳入败血症性休克组。共有 23 名患者在住院期间死亡,被纳入死亡组。随着症状的加重,年龄呈上升趋势,SIRS 组平均年龄为 56.86 岁,败血症组为 60.37 岁,败血症性休克组为 69.03 岁,死亡组为 71.04 岁(<0.04)。PCT 与复杂评分(SOFA、CCI 和 qSOFA)与尿脓毒症的发展之间存在统计学显著关联。死亡患者和败血症性休克患者的住院费用增加,而 SIRS 患者的住院费用明显降低。通过使用 ROC 曲线下面积 (AUC) 评估了区分尿脓毒症阶段的预测能力,发现 PCT(特异性 69.57%,敏感性 77.33%)、SOFA(特异性 91.33%,敏感性 76.82%)、qSOFA(特异性 91.30%,敏感性 74.17%)和 CCI(特异性 65.22%,敏感性 88.74%)对预测死亡风险的预测性非常好。qSOFA 的 AUC 值最佳(90.3%)。对于 SIRS 组,PCT(特异性 91.30%,敏感性 85.71%)和 SOFA(特异性 84.78%,敏感性 78.74%)、qSOFA 评分(特异性 84.78%,敏感性 76.34%)被证明在建立诊断方面具有相关性。对于败血症性休克组,qSOFA(特异性 92.5%,敏感性 82.71%)和 SOFA(特异性 97.5%,敏感性 77.44%)以及 PCT(特异性 80%,敏感性 85.61%)是统计学上显著的疾病定义变量。在将患者分类为败血症组的工具中存在明显的不足。所有变量的特异性都增加,但敏感性较低。这转化为假阴性诊断的风险。 : 尽管 SOFA 和 qSOFA 评分能够充分描述败血症性休克患者的病情,并且是死亡率的独立预后预测指标,但它们在诊断败血症方面并不准确。这些评分不应替代常规分诊方案。在我们的研究中,PCT 被证明是一种疾病定义标志物和死亡率的独立预后预测指标。CCI 大于 10 的患者有重要的合并症,应更积极地治疗,因为死亡率更高。