Division of Gastroenterology and Hepatology, Stanford University School of Medicine, Stanford, California.
Department of Medicine, Stanford University School of Medicine, Stanford, California.
Gastroenterology. 2018 Oct;155(4):1154-1163.e3. doi: 10.1053/j.gastro.2018.07.008. Epub 2018 Sep 1.
BACKGROUND & AIMS: Although treatment of hepatitis C virus (HCV) infection has improved, the prevalence of alcoholic liver disease (ALD) has been increasing, so we need an updated estimate of the burden and etiology-specific mortality of chronic liver diseases. We studied trends in age-standardized mortality of chronic liver diseases in adults at least 20 years old in the United States from 2007 through 2016.
We collected data from the US Census and National Center for Health Statistics mortality records and identified individuals with HCV infection, ALD, nonalcoholic fatty liver disease, or hepatitis B virus infection using ICD-10 codes. We obtained temporal mortality rate patterns using joinpoint trend analysis with estimates of annual percentage change (APC).
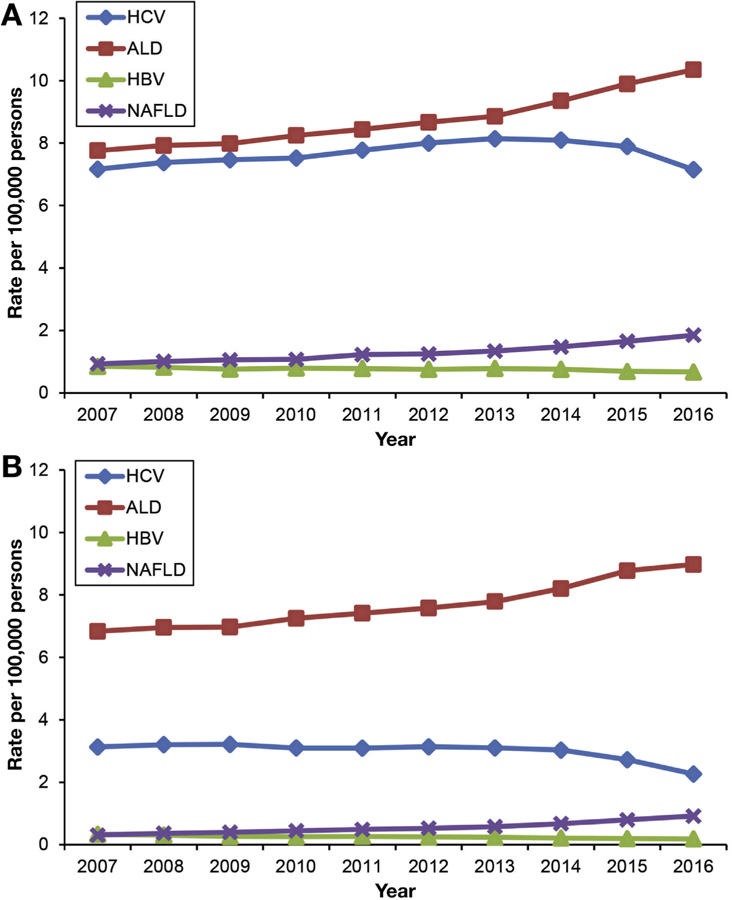
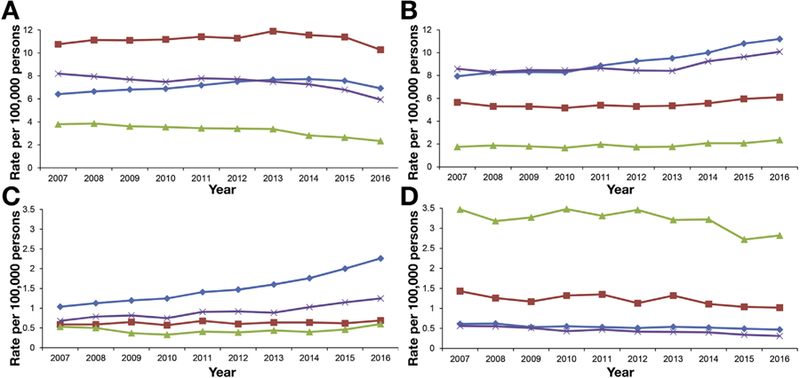
Age-standardized HCV-related mortality increased from 7.17 per 100,000 persons in 2007 to 8.14 per 100,000 persons in 2013, followed by a marked decrease in the time period at which patients began receiving treatment with direct-acting antiviral agents (from 8.09 per 100,000 persons in 2014 to 7.15 per 100,000 persons in 2016). The APC in HCV mortality increased 2.0%/year from 2007 through 2014 but decreased 6.4%/year from 2014 through 2016. In contrast, age-standardized mortality increased for ALD (APC 2.3% from 2007 through 2013 and APC 5.5% from 2013 through 2016) and nonalcoholic fatty liver disease (APC 6.1% from 2007 through 2013 and APC 11.3% from 2013 through 2016). Mortality related to hepatitis B virus decreased steadily from 2007 through 2016, with an average APC of -2.1% (95% CI -3.0 to -1.2). Etiology-based mortality in minority populations was higher. HCV-related mortality (per 100,000 persons) was highest in non-Hispanic blacks (10.28) and whites (6.92), followed by Hispanics (5.94), and lowest in non-Hispanic Asians (2.33). Non-Hispanic Asians had higher mortality for hepatitis B virus infection (2.82 per 100,000 vs 1.02 for non-Hispanic blacks and 0.47 for non-Hispanic whites).
In our population-based analysis of chronic liver disease mortality in the United States, the decrease in HCV-related mortality coincided with the introduction of direct-acting antiviral therapies, whereas mortality from ALD and nonalcoholic fatty liver disease increased during the same period. Minorities in the United States have disproportionately higher mortality related to chronic liver disease.
虽然丙型肝炎病毒(HCV)感染的治疗已经有所改善,但酒精性肝病(ALD)的患病率一直在上升,因此我们需要对慢性肝病的负担和病因特异性死亡率进行更新的估计。我们研究了 2007 年至 2016 年期间美国至少 20 岁成年人慢性肝病年龄标准化死亡率的趋势。
我们从美国人口普查和国家卫生统计中心的死亡率记录中收集数据,并使用 ICD-10 代码识别 HCV 感染、ALD、非酒精性脂肪性肝病或乙型肝炎病毒感染的个体。我们使用连接点趋势分析来获得时间死亡率模式,并估计每年百分比变化(APC)。
2007 年,与 HCV 相关的死亡率为每 100000 人 7.17 人,到 2013 年增加到每 100000 人 8.14 人,随后在开始使用直接作用抗病毒药物治疗的时间段内(2014 年每 100000 人 8.09 人至 2016 年每 100000 人 7.15 人)显著下降。2007 年至 2014 年,HCV 死亡率的 APC 每年增加 2.0%,但 2014 年至 2016 年每年下降 6.4%。相比之下,ALD(2007 年至 2013 年 APC 为 2.3%,2013 年至 2016 年 APC 为 5.5%)和非酒精性脂肪性肝病(2007 年至 2013 年 APC 为 6.1%,2013 年至 2016 年 APC 为 11.3%)的死亡率呈上升趋势。乙型肝炎病毒相关死亡率从 2007 年至 2016 年稳步下降,平均 APC 为-2.1%(95%CI-3.0 至-1.2)。少数族裔的病因死亡率更高。非西班牙裔黑人(每 100000 人 10.28 人)和白人(每 100000 人 6.92 人)的 HCV 相关死亡率(每 100000 人)最高,其次是西班牙裔(每 100000 人 5.94 人),非西班牙裔亚洲人(每 100000 人 2.33 人)最低。非西班牙裔亚洲人乙型肝炎病毒感染死亡率更高(每 100000 人 2.82 人,而非西班牙裔黑人为 1.02 人,非西班牙裔白人为 0.47 人)。
在我们对美国慢性肝病死亡率的基于人群的分析中,与 HCV 相关的死亡率下降与直接作用抗病毒疗法的引入同时发生,而同期 ALD 和非酒精性脂肪性肝病的死亡率上升。美国的少数族裔与慢性肝病相关的死亡率不成比例地更高。