Clinical Diagnostic Centre, 302 Military Hospital of China, Beijing, 100039, People's Republic of China.
Out-patient department, 302 Military Hospital of China, Beijing, 100039, People's Republic of China.
BMC Infect Dis. 2018 Aug 10;18(1):389. doi: 10.1186/s12879-018-3308-1.
It is difficult to diagnose ascites infection early in cirrhotic patients. The present study was to create and evaluate a new bioscore combined with PCT, sNFI and dCHC in the diagnosis of ascites infection in cirrhotic patients.
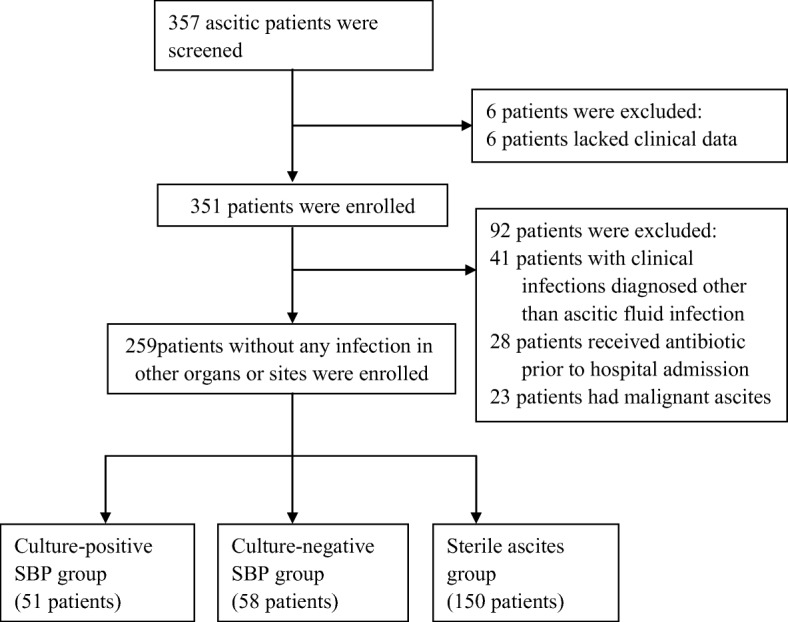
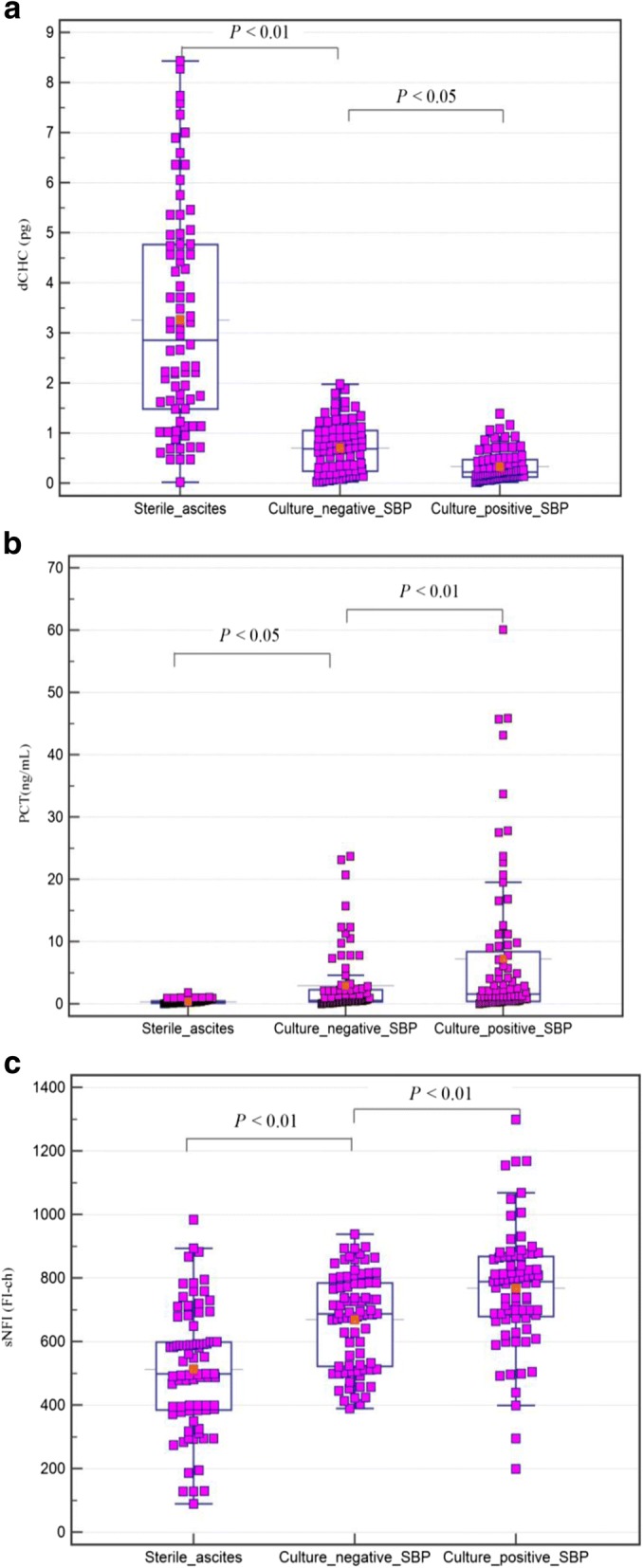
Two hundred and fifty-nine consecutive patients were enrolled; of which 51 patients were culture-positive spontaneous bacterial peritonitis (culture-positive SBP) and 58 patients were culture-negative SBP. The efficacy of procalcitonin(PCT), c-reactive protein (CRP), white blood cell (WBC), mean fluorescence intensity of mature neutrophils(sNFI) and difference in hemoglobin concentration between newly formed and mature red blood cells(dCHC) for diagnosing ascites infection was examined. These parameters were used to create a scoring system. The scoring system was analyzed by logistic regression analysis to determine which parameters were statistically different between ascites infection and non-ascites infection patients. Receiver operating characteristic curve (ROC) was used to analyze the diagnostic ability of bioscore for ascites infection.
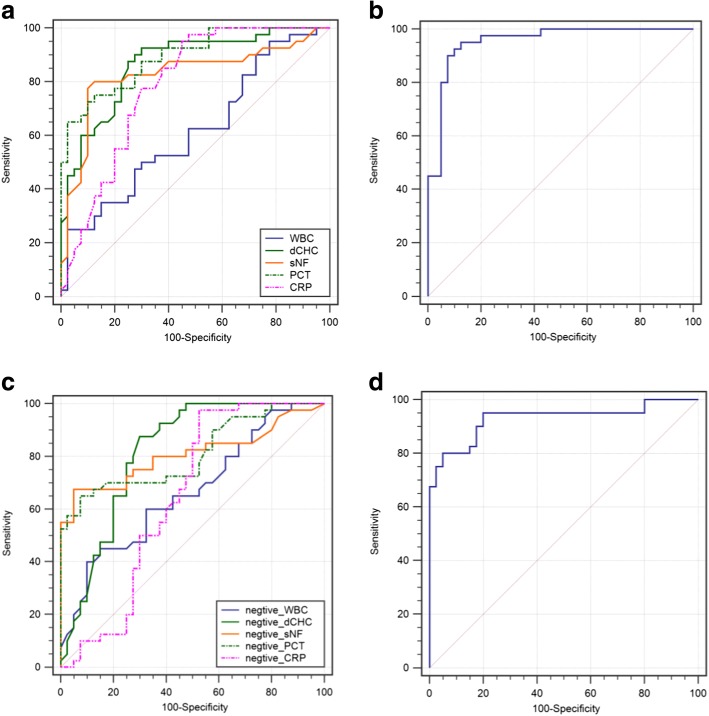
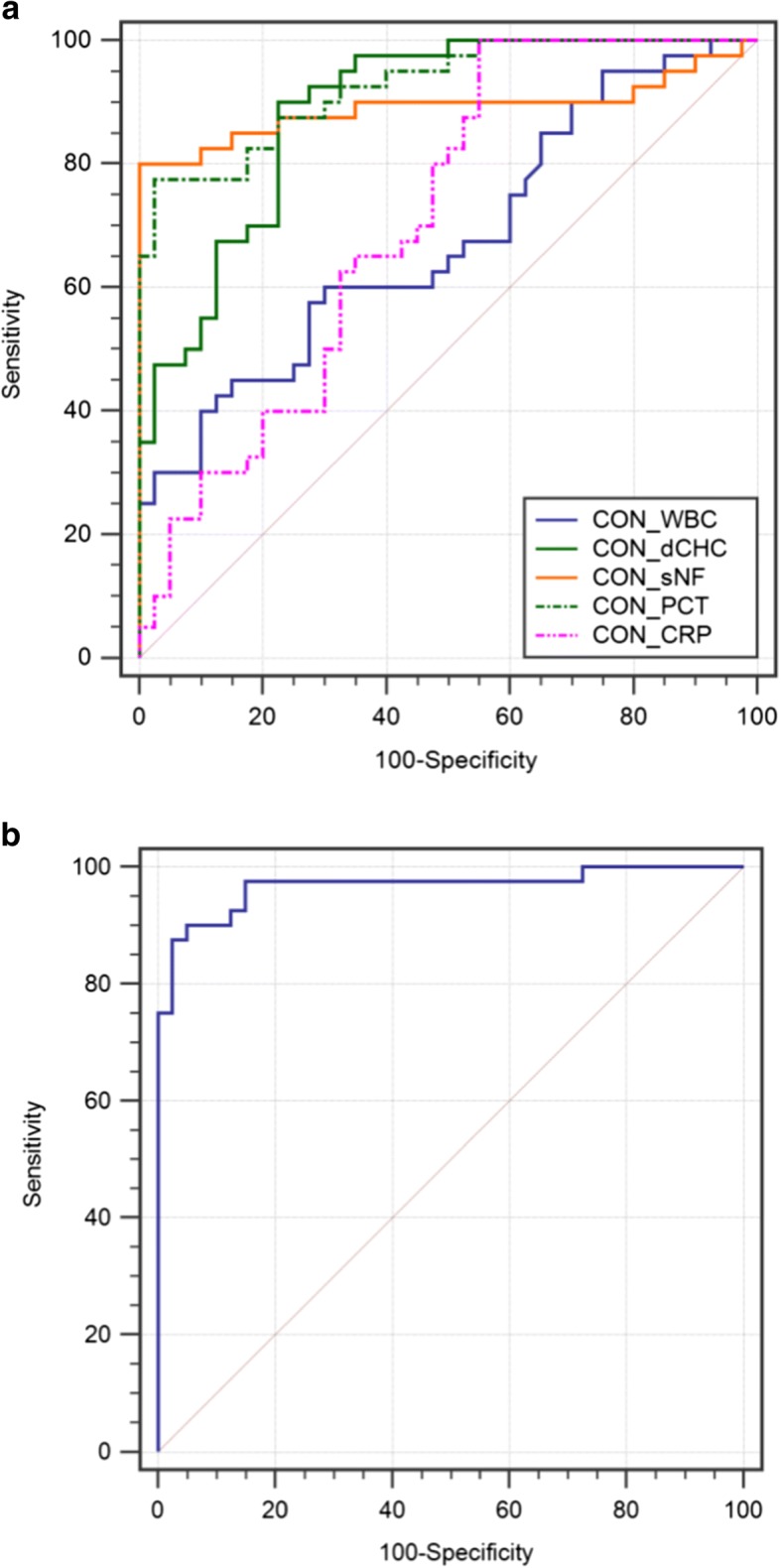
In ROC analysis, the area under the curves (AUC) for PCT was 0.852 (95% CI 0.803-0.921, P < 0.001), dCHC 0.837 (95% CI 0.773-0.923, P < 0.001), CRP 0.669 (95% CI 0.610-0.732, P = 0.0624), sNFI 0.838 (95% CI 0.777-0.903, P < 0.001), and WBC 0.624 (95% CI 0.500-0.722, P = 0.0881). Multivariate analysis revealed PCT, dCHC and sNFI to be statistically significant. The combination of these three parameters in the bioscore had an AUC of 0.937 (95% CI 0.901-0.994, P < 0.001). A bioscore of ≥3.40 was considered to be statistically significant in making a positive diagnosis of ascites infection. In different groups of ascites infection, bioscore also shown a high diagnostic value of AUC was 0.947(95% CI 0.882-0.988, P < 0.001) and 0.929 (95% CI 0.869-0.974, P < 0.001) for culture-positive SBP and culture-negative SBP group respectively.
The composite markers of combining PCT, dCHC and sNFI could be a valuable diagnostic score to early diagnose ascites infection in patients with cirrhosis.
在肝硬化患者中,早期诊断腹水感染较为困难。本研究旨在建立并评估一种新的生物标志物评分,联合降钙素原(PCT)、sNFI 和 dCHC,用于诊断肝硬化患者的腹水感染。
连续纳入 259 例患者;其中 51 例为培养阳性自发性细菌性腹膜炎(culture-positive SBP),58 例为培养阴性 SBP。检测 PCT、C 反应蛋白(CRP)、白细胞(WBC)、成熟中性粒细胞的平均荧光强度(sNFI)和新形成与成熟红细胞之间的血红蛋白浓度差异(dCHC)在诊断腹水感染中的效能。使用这些参数创建评分系统。通过逻辑回归分析对评分系统进行分析,以确定腹水感染和非腹水感染患者之间统计学上有差异的参数。采用受试者工作特征曲线(ROC)分析生物标志物评分对腹水感染的诊断能力。
在 ROC 分析中,PCT 的曲线下面积(AUC)为 0.852(95%CI 0.803-0.921,P<0.001),dCHC 为 0.837(95%CI 0.773-0.923,P<0.001),CRP 为 0.669(95%CI 0.610-0.732,P=0.0624),sNFI 为 0.838(95%CI 0.777-0.903,P<0.001),WBC 为 0.624(95%CI 0.500-0.722,P=0.0881)。多变量分析显示 PCT、dCHC 和 sNFI 具有统计学意义。这三个参数联合的生物标志物评分 AUC 为 0.937(95%CI 0.901-0.994,P<0.001)。生物标志物评分≥3.40 被认为是腹水感染阳性诊断的统计学显著标准。在不同的腹水感染组中,生物标志物评分的 AUC 也具有较高的诊断价值,分别为 0.947(95%CI 0.882-0.988,P<0.001)和 0.929(95%CI 0.869-0.974,P<0.001),用于培养阳性 SBP 和培养阴性 SBP 组。
联合 PCT、dCHC 和 sNFI 的复合标志物可能是一种有价值的诊断评分,用于早期诊断肝硬化患者的腹水感染。