Arthritis Research UK Centre for Epidemiology, Division of Musculoskeletal & Dermatological Sciences, Manchester, UK.
Arthritis Research UK Centre for Genetics and Genomics, Division of Musculoskeletal & Dermatological Sciences, School of Biological Sciences, Faculty of Biology, Medicine and Health, The University of Manchester, Manchester Academic Health Science Centre, Manchester, UK.
Rheumatology (Oxford). 2018 Dec 1;57(12):2172-2182. doi: 10.1093/rheumatology/key224.
To compare the prevalence and incidence of chronic co-morbidities in people with inflammatory rheumatic and musculoskeletal diseases (iRMDs), and to determine whether the prevalent co-morbidities are associated with physical activity levels in people with iRMDs and in those without iRMDs.
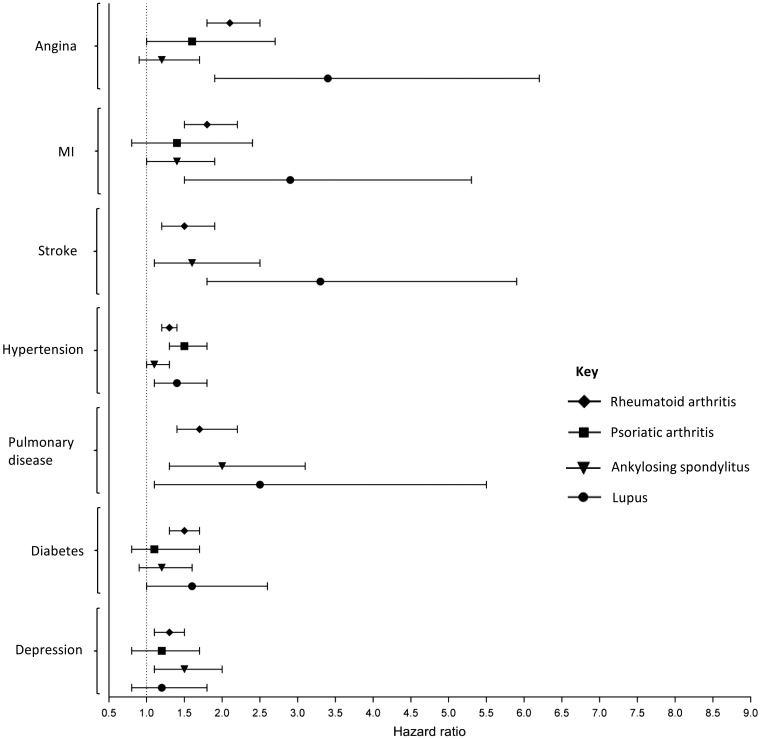
Participants were recruited to the UK Biobank; a population-based cohort. Data were collected about demographics, physical activity, iRMDs (RA, PsA, AS, SLE) and other chronic conditions, including angina, myocardial infarction, stroke, hypertension, pulmonary disease, diabetes and depression. The standardized prevalence of co-morbidities in people with iRMDs was calculated. Cox regression was used to determine the relationship between the presence of an iRMD and an incident co-morbidity. The relationship between the presence (versus absence) of a (co-)morbidity and physical activity level (low, moderate, high) in people with iRMDs and in those without was assessed using multinomial logistic regression.
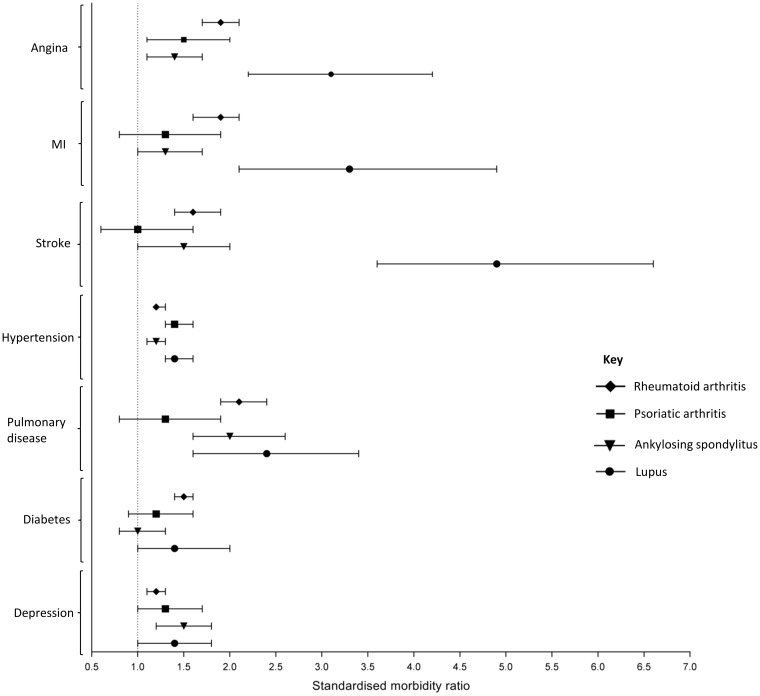
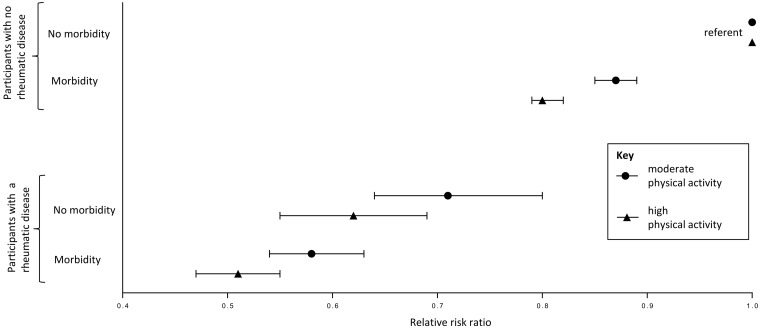
A total of 488 991 participants were included. The estimated prevalence of each co-morbidity was increased in participants with an iRMD, compared with in those without, particularly for stroke in participants with SLE (standardized morbidity ratio (95% CI), 4.9 (3.6, 6.6). Compared with people with no iRMD and no morbidity, the odds ratios (95% CI) for moderate physical activity were decreased for: no iRMD and morbidity, 0.87 (0.85, 0.89); iRMD and no co-morbidity, 0.71 (0.64, 0.80); and iRMD and co-morbidity, 0.58 (0.54, 0.63).
Having a (co-)morbidity is associated with reduced physical activity in the general population, and to a greater extent in participants with an iRMD. Optimal management of both iRMDs and co-morbidities may help to reduce their impact on physical activity.
比较患有炎症性风湿和肌肉骨骼疾病(iRMDs)的人群中慢性合并症的患病率和发病率,并确定 iRMDs 患者和无 iRMDs 患者的现有合并症是否与身体活动水平相关。
参与者被招募到英国生物银行(UK Biobank);这是一个基于人群的队列。收集了有关人口统计学、身体活动、iRMDs(RA、PsA、AS、SLE)和其他慢性疾病(包括心绞痛、心肌梗死、中风、高血压、肺部疾病、糖尿病和抑郁症)的数据。计算了患有 iRMDs 的人群中合并症的标准化患病率。使用 Cox 回归确定存在 iRMD 与新发合并症之间的关系。使用多项逻辑回归评估患有 iRMDs 的人群和无 iRMDs 的人群中(合并症的)存在(与不存在)与身体活动水平(低、中、高)之间的关系。
共纳入 488991 名参与者。与无 iRMDs 的参与者相比,患有 iRMDs 的参与者的每种合并症的估计患病率均有所增加,尤其是 SLE 患者的中风(标准化发病率比(95%CI),4.9(3.6,6.6)。与无 iRMDs 且无合并症的人群相比,中度身体活动的优势比(95%CI)为:无 iRMDs 且有合并症,0.87(0.85,0.89);有 iRMDs 且无合并症,0.71(0.64,0.80);有 iRMDs 且有合并症,0.58(0.54,0.63)。
在一般人群中,患有(合并症)与身体活动减少有关,在患有 iRMDs 的人群中更为明显。优化 iRMDs 和合并症的管理可能有助于降低它们对身体活动的影响。