Exercise Biochemistry Laboratory, School of Kinesiology, Western University, London, ON, Canada.
Lawson Health Research Institute, London, ON, Canada.
J Diabetes Res. 2018 Jul 5;2018:8485624. doi: 10.1155/2018/8485624. eCollection 2018.
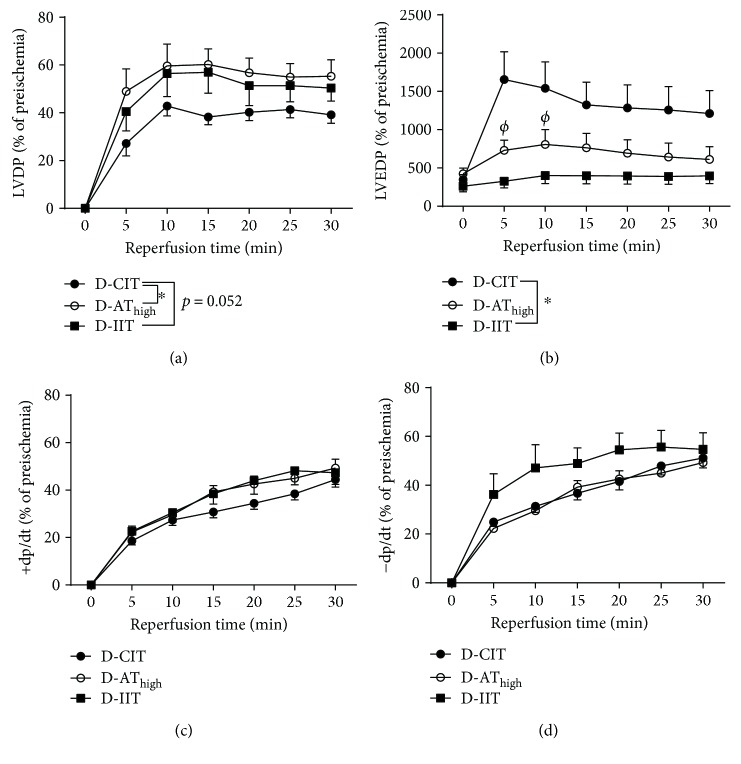
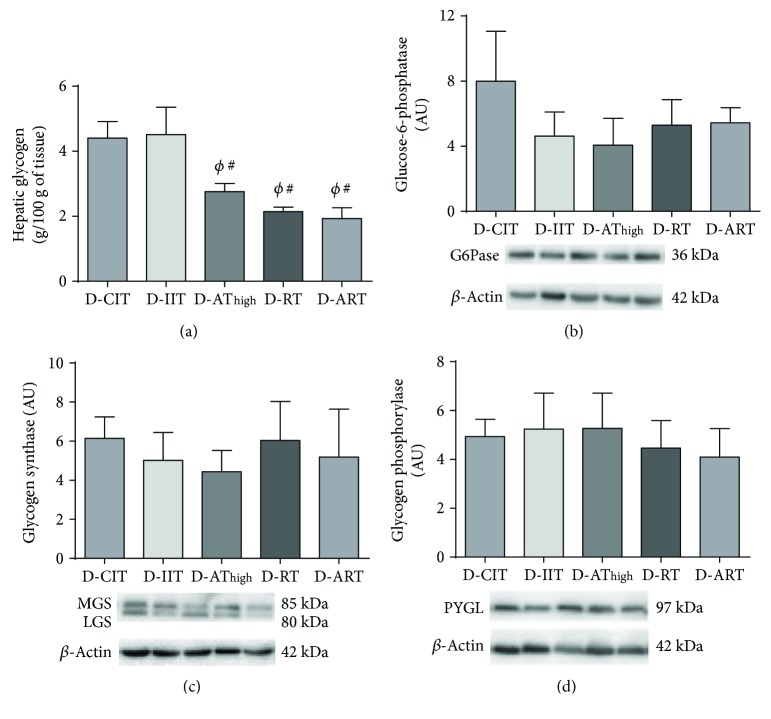
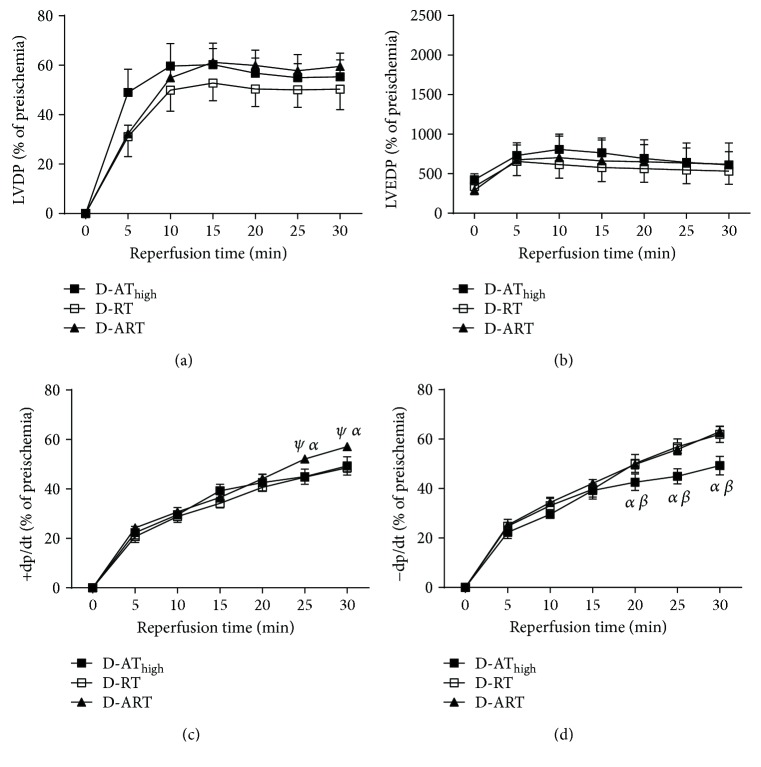
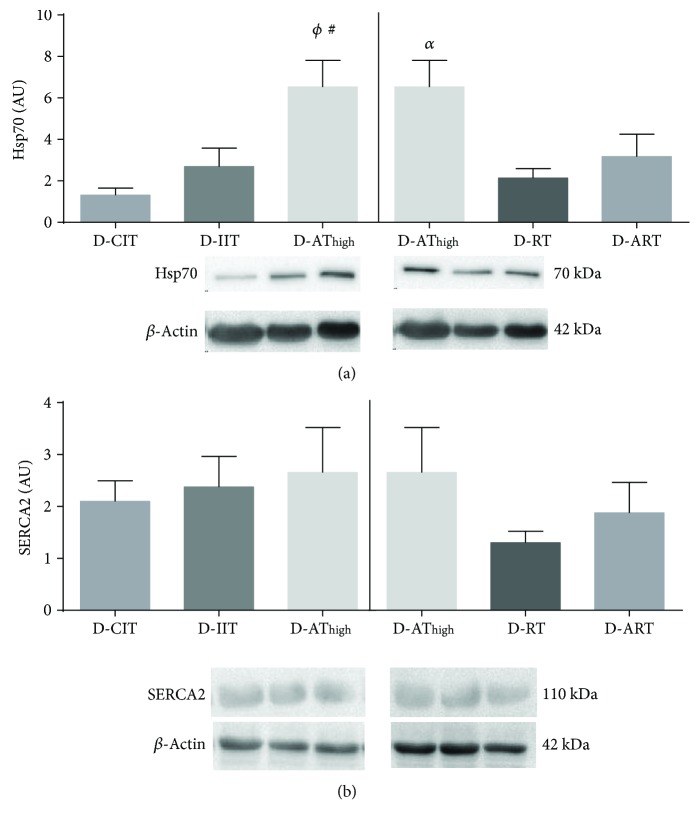
Intensive insulin therapy (IIT; 4-7 mmol/L) is the preferred treatment for type 1 diabetes mellitus (T1DM) patients to reduce the risk of cardiovascular disease (CVD). However, this treatment strategy has been questioned as it is accompanied with a sedentary lifestyle leading to weight gain and insulin resistance. T1DM patients who partake in high-intensity aerobic training (AT) to reduce CVD often utilize conventional insulin therapy (CIT; 9-15 mmol/L) to offset the risk of hypoglycemia. Moreover, exercise modalities incorporating resistance training (RT) have been shown to further reduce this risk. The purpose of this investigation was twofold: (1) to determine if CIT paired with AT results in larger cardioprotection from an ischemia-reperfusion (I-R) injury than IIT and (2) to establish if the integration of RT with AT (ART) results in similar cardioprotection as AT. Diabetic (D) male Sprague-Dawley rats were divided into D-IIT ( = 12), D-CIT ( = 12), D-AT ( = 8), D-RT ( = 8), and D-ART ( = 8). T1DM was induced with streptozotocin, and blood glucose was adjusted with insulin. D-AT occurred on a treadmill (27 m/min; 1 hr), D-RT performed weighted ladder climbs, and D-ART alternated daily between AT and RT. Exercise occurred 5 days/wk for 12 wks. This investigation demonstrates that cardioprotection following an I-R injury was similar between D-AT and D-IIT. This cardioprotection is not exercise-specific, and each provides unique advantages. D-AT leads to improved glycemia while insulin sensitivity was enhanced following resistance exercises. Thus, exercise is an effective means to elicit cardioprotection in T1DM. However, in addition to glycemia, other factors should be considered when tailoring an exercise program for T1DM patients.
强化胰岛素治疗(IIT;4-7mmol/L)是治疗 1 型糖尿病(T1DM)患者以降低心血管疾病(CVD)风险的首选治疗方法。然而,这种治疗策略受到了质疑,因为它伴随着久坐的生活方式,导致体重增加和胰岛素抵抗。为了降低 CVD 风险,参与高强度有氧运动(AT)的 T1DM 患者通常会使用常规胰岛素治疗(CIT;9-15mmol/L)来抵消低血糖的风险。此外,已经证明结合抗阻训练(RT)的运动方式可以进一步降低这种风险。本研究的目的有两个:(1)确定 CIT 联合 AT 是否比 IIT 产生更大的缺血再灌注(I-R)损伤的心脏保护作用;(2)确定 AT 与 RT 的整合(ART)是否产生与 AT 相似的心脏保护作用。糖尿病(D)雄性 Sprague-Dawley 大鼠分为 D-IIT(n=12)、D-CIT(n=12)、D-AT(n=8)、D-RT(n=8)和 D-ART(n=8)。T1DM 用链脲佐菌素诱导,并用胰岛素调整血糖。D-AT 在跑步机上进行(27m/min;1 小时),D-RT 进行负重爬梯,D-ART 每天交替进行 AT 和 RT。每周运动 5 天,共 12 周。本研究表明,I-R 损伤后的心脏保护作用在 D-AT 和 D-IIT 之间相似。这种心脏保护作用不是运动特异性的,每种方法都有独特的优势。D-AT 可改善血糖,而抗阻运动后胰岛素敏感性增强。因此,运动是诱发 T1DM 心脏保护的有效手段。然而,在为 T1DM 患者制定运动计划时,除了血糖外,还应考虑其他因素。