Department of Gynecology and Obstetrics, Saarland University Medical Center, Homburg/Saar, Germany.
Department of Pediatric Cardiology, Saarland University Medical Center, Homburg/Saar, Germany.
PLoS One. 2018 Aug 17;13(8):e0202406. doi: 10.1371/journal.pone.0202406. eCollection 2018.
Soluble suppression of tumorogenicity 2 (sST2) has been shown to be of prognostic value in patients with chronic and acute left heart failure. The present study aims to assess the predictive value of sST2 levels in adult patients with complex congenital heart disease (CHD).
In 169 consecutive patients with complex CHD and a mean age of 28.2 ± 12.0 years, sST2 levels were compared to 32 healthy controls and associated with clinical status as well as the occurrence of major adverse cardiac events (MACE). Mean follow-up time was 35.6 ± 24.9 months.
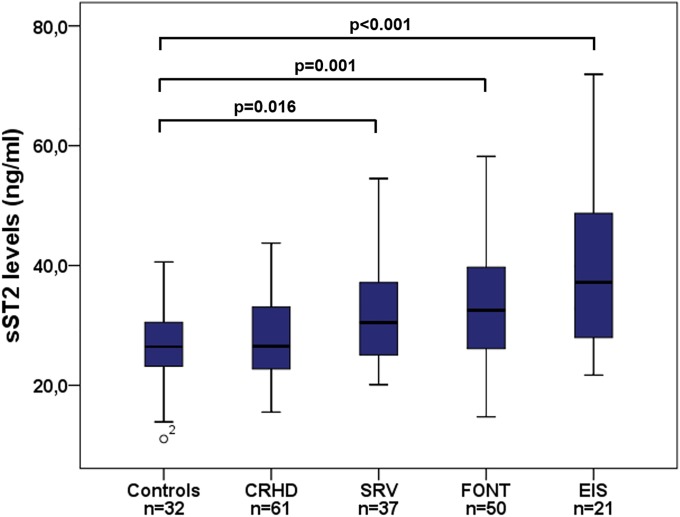
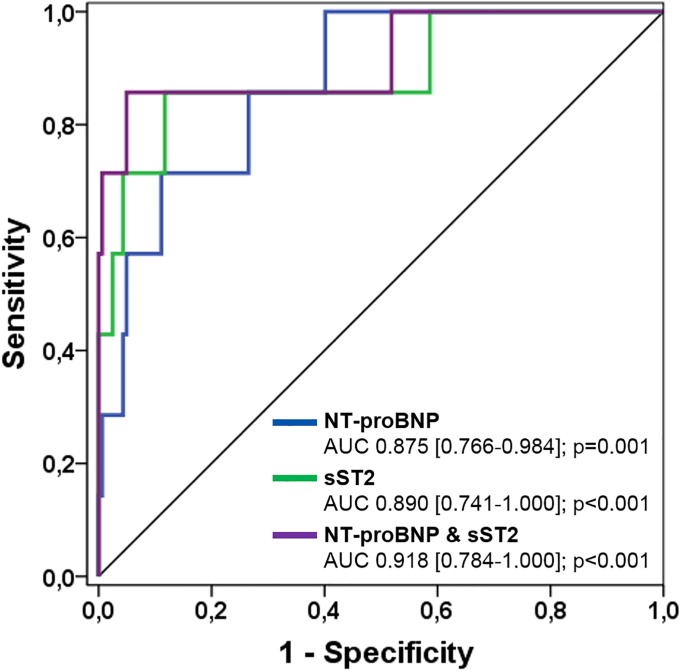
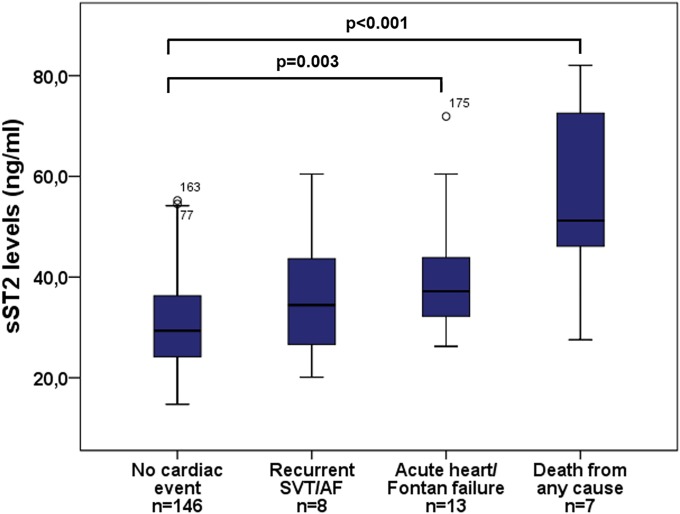
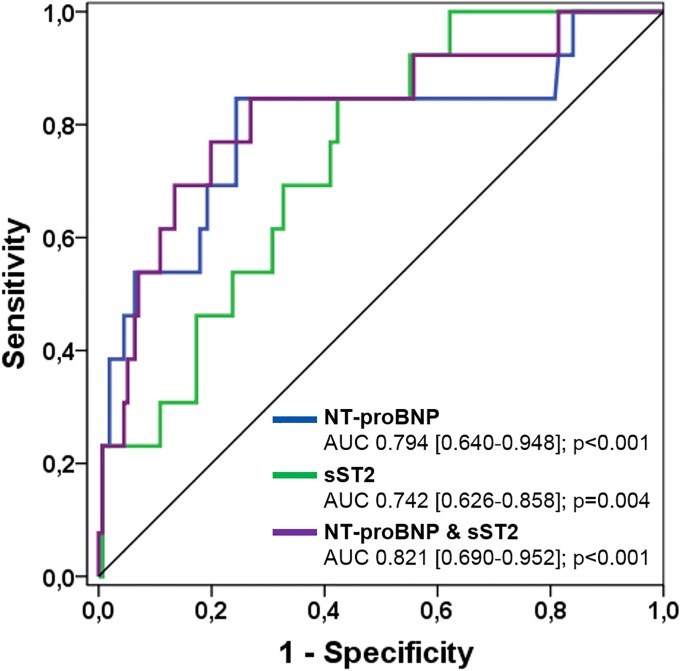
In CHD patients, median sST2 levels were 29.7 ng/ml compared to 26.4 ng/ml in healthy controls (p = 0.007) and increased with different types of CHD and the severity of MACE. According to ROC analysis, the most important predictors of acute heart/Fontan failure were NYHA class III/IV (AUC 0.804, p<0.001, CI 0.668-0.941), NT-proBNP levels (AUC 0.794, p<0.001, CI 0.640-0.948), γGT levels (AUC 0.793, p<0.001, CI 0.678-0.909) and sST2 levels (AUC 0.742, p = 0.004, CI 0.626-0.858), with NYHA class III/IV as the strongest independent predictor (p<0.001). All-cause mortality was best predicted by sST2 levels (AUC 0.890, p<0.001, CI 0.741-1.000), NT-proBNP levels (AUC 0.875, p = 0.001, CI 0.766-0.984) and NYHA class III/IV (AUC 0.837, p = 0.003, CI 0.655-1.000) with sST2 as the strongest independent predictor (p<0.001). Moreover, AUC increased to 0.918 combining both biomarkers and net reclassification improved with the addition of sST2.
In patients with complex CHD, sST2 may have additive value to natriuretic peptides for the prediction of all-cause mortality.
可溶性抑制肿瘤发生 2 型(sST2)已被证明在慢性和急性左心衰竭患者中具有预后价值。本研究旨在评估 sST2 水平在成人复杂先天性心脏病(CHD)患者中的预测价值。
在 169 例连续的复杂 CHD 患者中,平均年龄为 28.2±12.0 岁,将 sST2 水平与 32 名健康对照者进行比较,并与临床状况以及主要不良心脏事件(MACE)的发生相关联。平均随访时间为 35.6±24.9 个月。
在 CHD 患者中,中位数 sST2 水平为 29.7ng/ml,而健康对照组为 26.4ng/ml(p=0.007),并且随着 CHD 类型和 MACE 严重程度的不同而增加。根据 ROC 分析,急性心脏/Fontan 衰竭的最重要预测因素是 NYHA 分级 III/IV(AUC 0.804,p<0.001,CI 0.668-0.941)、NT-proBNP 水平(AUC 0.794,p<0.001,CI 0.640-0.948)、γGT 水平(AUC 0.793,p<0.001,CI 0.678-0.909)和 sST2 水平(AUC 0.742,p=0.004,CI 0.626-0.858),其中 NYHA 分级 III/IV 为最强的独立预测因素(p<0.001)。全因死亡率最好由 sST2 水平预测(AUC 0.890,p<0.001,CI 0.741-1.000)、NT-proBNP 水平(AUC 0.875,p=0.001,CI 0.766-0.984)和 NYHA 分级 III/IV(AUC 0.837,p=0.003,CI 0.655-1.000),其中 sST2 为最强的独立预测因素(p<0.001)。此外,结合两种生物标志物后 AUC 增加至 0.918,并且添加 sST2 后净重新分类得到改善。
在复杂 CHD 患者中,sST2 可能对 natriuretic 肽具有附加价值,可用于预测全因死亡率。