Medical Intensive Care Unit, iCAN, Institute of Cardiometabolism and Nutrition, Hôpital de la Pitié-Salpêtrière, Assistance Publique-Hôpitaux de Paris, Sorbonne University , Paris 6, 47, bd de l'Hôpital, 75651, Paris Cedex 13, France.
Laboratory of Microbiology, Hôpital de la Pitié-Salpêtrière, Assistance Publique-Hôpitaux de Paris, Sorbonne University , Paris 6, 47, bd de l'Hôpital, 75651, Paris Cedex 13, France.
Crit Care. 2018 Aug 19;22(1):199. doi: 10.1186/s13054-018-2122-x.
Amikacin infusion requires targeting a peak serum concentration (C) 8-10 times the minimal inhibitory concentration, corresponding to a C of 60-80 mg/L for the least susceptible bacteria to theoretically prevent therapeutic failure. Because drug pharmacokinetics on extracorporeal membrane oxygenation (ECMO) are challenging, we undertook this study to assess the frequency of insufficient amikacin C in critically ill patients on ECMO and to identify relative risk factors.
This was a prospective, observational, monocentric study in a university hospital. Patients on ECMO who received an amikacin loading dose for suspected Gram-negative infections were included. The amikacin loading dose of 25 mg/kg total body weight was administered intravenously and C was measured 30 min after the end of the infusion. Independent predicators of C < 60 mg/L after the first amikacin infusion were identified with mixed-model multivariable analyses. Various dosing simulations were performed to assess the probability of reaching 60 mg/L < C < 80 mg/L.
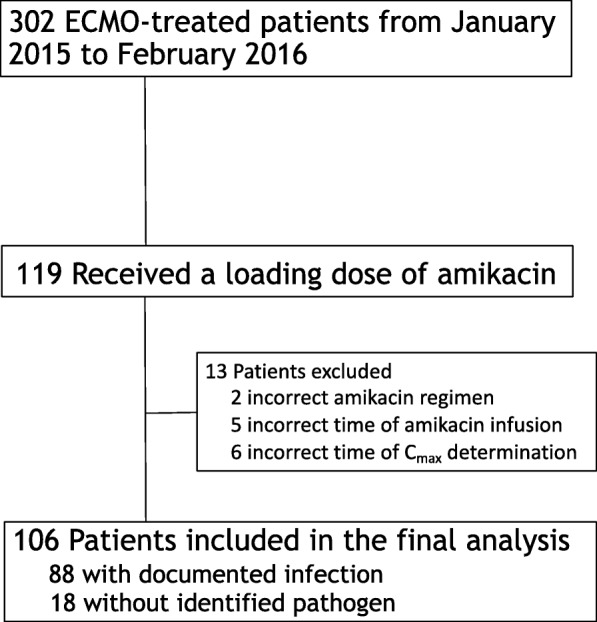
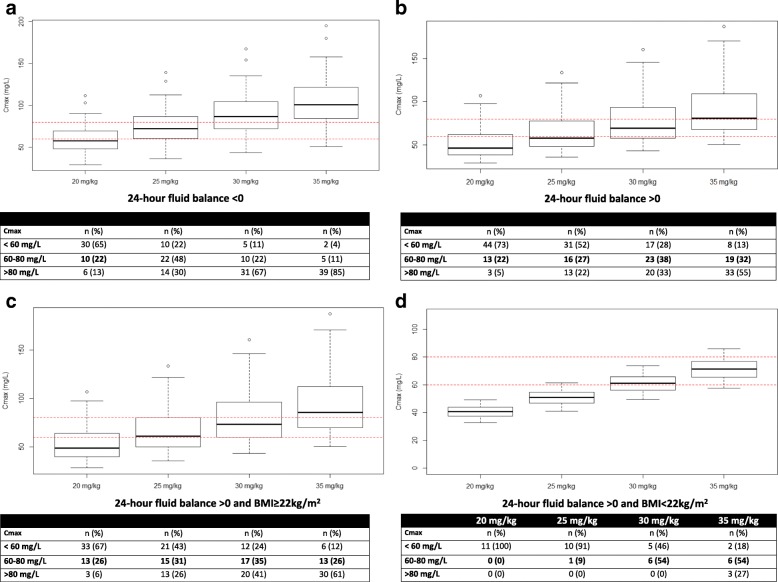
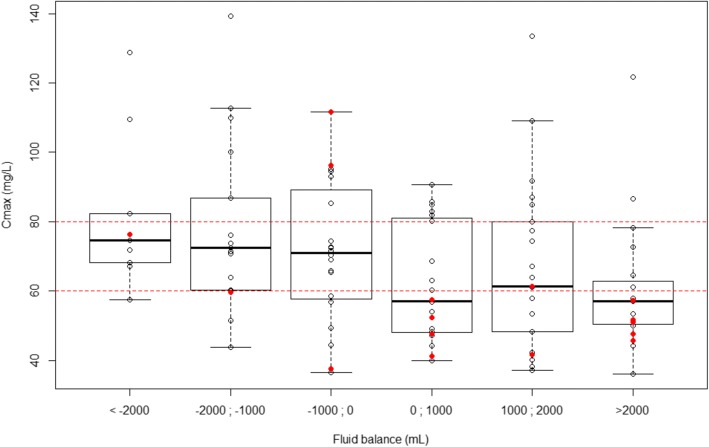
A total of 106 patients on venoarterial ECMO (VA-ECMO) (68%) or venovenous-ECMO (32%) were included. At inclusion, their median (1st; 3rd quartile) Sequential Organ-Failure Assessment score was 15 (12; 18) and 54 patients (51%) were on renal replacement therapy. Overall ICU mortality was 54%. C was < 60 mg/L in 41 patients (39%). Independent risk factors for amikacin under-dosing were body mass index (BMI) < 22 kg/m and a positive 24-h fluid balance. Using dosing simulation, increasing the amikacin dosing regimen to 30 mg/kg and 35 mg/kg of body weight when the 24-h fluid balance is positive and the BMI is ≥ 22 kg/m or < 22 kg/m (Table 3), respectively, would have potentially led to the therapeutic target being reached in 42% of patients while reducing under-dosing to 23% of patients.
ECMO-treated patients were under-dosed for amikacin in one third of cases. Increasing the dose to 35 mg/kg of body weight in low-BMI patients and those with positive 24-h fluid balance on ECMO to reach adequate targeted concentrations should be investigated.
阿米卡星输注需要将血清峰浓度(C)靶向设定为最小抑菌浓度的 8-10 倍,对于理论上防止治疗失败的最易感细菌,C 应达到 60-80mg/L。由于体外膜肺氧合(ECMO)的药物药代动力学具有挑战性,因此我们进行了这项研究,以评估 ECMO 治疗的危重症患者中阿米卡星 C 浓度不足的频率,并确定相关的危险因素。
这是一项在大学医院进行的前瞻性、观察性、单中心研究。纳入接受疑似革兰氏阴性感染的阿米卡星负荷剂量治疗的 ECMO 患者。静脉给予 25mg/kg 总体重的阿米卡星负荷剂量,在输注结束后 30 分钟测量 C。使用混合模型多变量分析确定首次阿米卡星输注后 C<60mg/L 的独立预测因子。进行了各种给药模拟,以评估达到 60mg/L<C<80mg/L 的概率。
共纳入 106 例接受静脉-动脉 ECMO(VA-ECMO)(68%)或静脉-静脉 ECMO(32%)的患者。纳入时,他们的序贯器官衰竭评估(SOFA)评分中位数(第 1 四分位数;第 3 四分位数)为 15(12;18),54 例(51%)患者正在接受肾脏替代治疗。总体 ICU 死亡率为 54%。41 例(39%)患者的 C<60mg/L。阿米卡星剂量不足的独立危险因素是 BMI<22kg/m2 和 24 小时正液体平衡。使用给药模拟,如果 24 小时液体平衡为正且 BMI≥22kg/m2 或<BMI<22kg/m2(表 3),将阿米卡星剂量方案增加至 30mg/kg 和 35mg/kg 体重,将有可能使 42%的患者达到治疗目标,同时将剂量不足的患者减少至 23%。
三分之一的 ECMO 治疗患者的阿米卡星剂量不足。应研究在 ECMO 治疗的低 BMI 患者和有 24 小时正液体平衡的患者中,将剂量增加至 35mg/kg 体重,以达到足够的目标浓度。