Hald Stine Munk, Kring Sloth Christine, Hey Sabine Morris, Madsen Charlotte, Nguyen Nina, García Rodríguez Luis Alberto, Al-Shahi Salman Rustam, Möller Sören, Poulsen Frantz Rom, Pottegård Anton, Gaist David
Department of Neurology, Odense University Hospital, Odense, Denmark,
Department of Clinical Research, Faculty of Health Sciences, University of Southern Denmark, Odense, Denmark,
Clin Epidemiol. 2018 Aug 7;10:941-948. doi: 10.2147/CLEP.S167576. eCollection 2018.
The purpose of this study is to establish the validity of intracerebral hemorrhage (ICH) diagnoses in the Danish Stroke Registry (DSR) and the Danish National Patient Registry (DNPR).
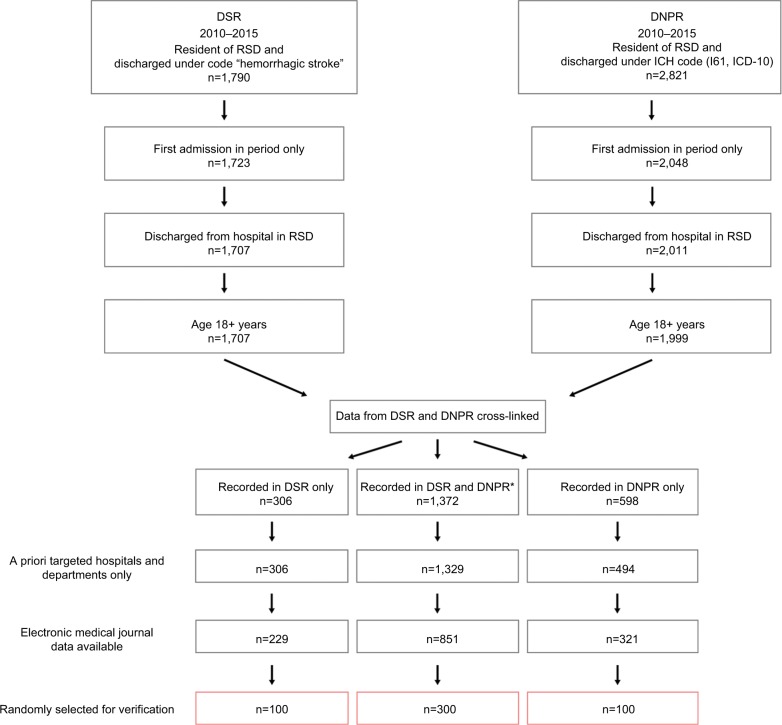
We estimated the positive predictive value (PPV) of ICH diagnoses for a sample of 500 patients from the DSR (patients recorded under ICH diagnosis) and DNPR (International Classification of Diseases, version 10, code I61) during 2010-2015, using discharge summaries and brain imaging reports (minimal data). We estimated PPVs for any ICH (a-ICH) and spontaneous ICH (s-ICH) alone. Furthermore, we assessed PPVs according to whether patients were recorded in both or only one of the registries. Finally, in a subsample with ICH diagnoses with access to full medical records and original imaging studies (extensive data, n=100), we compared s-ICH diagnosis and hemorrhage location after use of extensive vs minimal data.
In the DSR, the PPVs were 94% (95% CI, 91%-96%) for a-ICH and 85% (95% CI, 81%-88%) for s-ICH. In the DNPR, the PPVs were 88% (95% CI, 84%-91%) for a-ICH and 75% (95% CI, 70%-79%) for s-ICH. PPVs for s-ICH for patients recorded in both registries, DSR only, and DNPR only were 86% (95% CI, 82-99), 80% (95%CI, 71-87), and 49% (95%CI, 39-59), respectively. Evaluation of extensive vs minimal data verified s-ICH diagnosis in 98% and hemorrhage location in 94%.
The validity of a-ICH diagnoses in DSR and DNPR is sufficiently high to support their use in epidemiologic studies. For s-ICH, validity was high in DSR. In DNPR, s-ICH validity was lower, markedly so for the small subgroup of patients only recorded in this registry. Minimal data including discharge summaries and brain imaging reports were feasible and valid for identifying ICH location.
本研究旨在确定丹麦卒中登记处(DSR)和丹麦国家患者登记处(DNPR)中脑出血(ICH)诊断的有效性。
我们利用出院小结和脑部影像报告(最少数据),对2010 - 2015年期间来自DSR(记录为ICH诊断的患者)和DNPR(国际疾病分类第10版,编码I61)的500例患者样本,估计ICH诊断的阳性预测值(PPV)。我们分别估计了所有ICH(a - ICH)和自发性ICH(s - ICH)的PPV。此外,我们根据患者是记录在两个登记处还是仅记录在其中一个登记处来评估PPV。最后,在一个可获取完整病历和原始影像研究(详尽数据,n = 100)的ICH诊断子样本中,我们比较了使用详尽数据与最少数据后的s - ICH诊断及出血部位。
在DSR中,a - ICH的PPV为94%(95%CI,91% - 96%),s - ICH的PPV为85%(95%CI,81% - 88%)。在DNPR中,a - ICH的PPV为88%(95%CI,84% - 91%),s - ICH的PPV为75%(95%CI,70% - 79%)。记录在两个登记处、仅记录在DSR以及仅记录在DNPR中的患者,其s - ICH的PPV分别为86%(95%CI,82 - 99)、80%(95%CI,71 - 87)和49%(95%CI,39 - 59)。对详尽数据与最少数据的评估显示,s - ICH诊断的验证率为98%,出血部位的验证率为94%。
DSR和DNPR中a - ICH诊断的有效性足够高,足以支持其在流行病学研究中的应用。对于s - ICH,DSR中的有效性较高。在DNPR中,s - ICH的有效性较低,仅记录在该登记处的小部分患者尤为明显。包括出院小结和脑部影像报告在内的最少数据对于确定ICH部位是可行且有效的。