Ahmed Armin, Azim Afzal
1Department of Critical Care Medicine, King George Medical University, Lucknow, 226003 India.
2Department of Critical Care Medicine, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, 226014 India.
J Intensive Care. 2018 Aug 13;6:49. doi: 10.1186/s40560-018-0318-4. eCollection 2018.
Endotracheal intubation in critically ill is a high-risk procedure requiring significant expertise in airway handling as well as understanding of pathophysiology of the disease process.
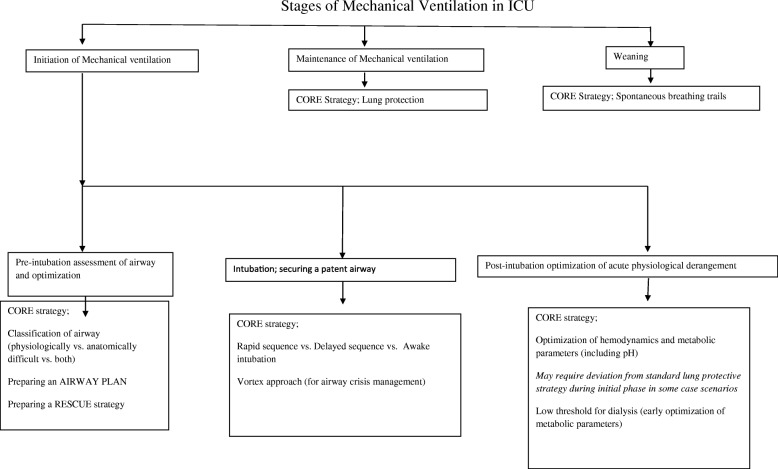
Critically ill patients are prone for hypotension and hypoxemia in the immediate post-intubation phase due to blunting of compensatory sympathetic response. Preoxygenation without NIV is frequently suboptimal, as alveolar flooding cause loss of alveolar capillary interface in many of these patients. All these factors, along with relative fluid deficit, neuromuscular fatigue and coexistent organ dysfunction lead to physiologically difficult airway. Airway in ICU can be classified as anatomically difficult, physiologically difficult and anatomically as well as physiologically difficult. Though rapid sequence intubation is the recommended method for securing airway in these patients, other methods like delayed sequence intubation awake intubation and double setup approach can be used in specific subgroups. Further research is needed in this field to set guidelines and fine tune airway management for patients with specific organ failure or dysfunction.
Airway in ICU should be managed according to the physiological as well as the anatomical abnormalities.
危重症患者的气管插管是一项高风险操作,需要在气道处理方面具备专业技能,同时要了解疾病过程的病理生理学。
由于代偿性交感反应减弱,危重症患者在插管后即刻易发生低血压和低氧血症。在许多此类患者中,由于肺泡充盈导致肺泡毛细血管界面丧失,不使用无创通气的预给氧往往效果欠佳。所有这些因素,连同相对液体不足、神经肌肉疲劳和并存的器官功能障碍,导致气道生理状况复杂。重症监护病房(ICU)的气道可分为解剖结构复杂、生理状况复杂以及解剖结构和生理状况均复杂。尽管快速顺序诱导插管是这些患者确保气道安全的推荐方法,但在特定亚组中可采用其他方法,如延迟顺序诱导插管、清醒插管和双设备法。该领域需要进一步研究以制定指南并优化针对特定器官衰竭或功能障碍患者的气道管理。
ICU的气道管理应根据生理和解剖异常情况进行。