Orr Carl K, Najm Aurelie, Young Francis, McGarry Trudy, Biniecka Monika, Fearon Ursula, Veale Douglas J
Dublin Academic Medical Centre, Centre for Arthritis and Rheumatic Diseases, University College Dublin, Dublin, Ireland.
Molecular Rheumatology Research Group, Trinity Biomedical Sciences Institute, Trinity College, Dublin, Ireland.
Front Med (Lausanne). 2018 Aug 3;5:185. doi: 10.3389/fmed.2018.00185. eCollection 2018.
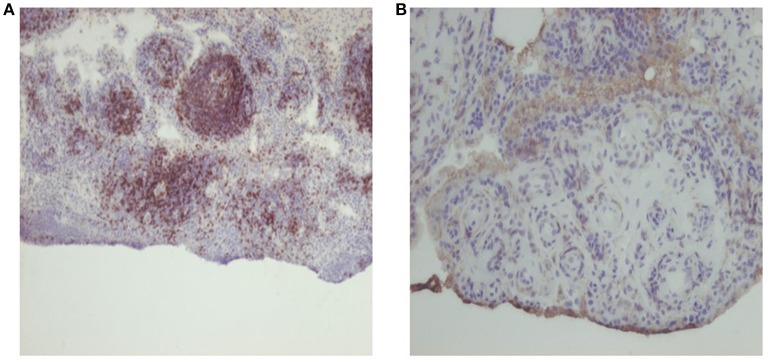
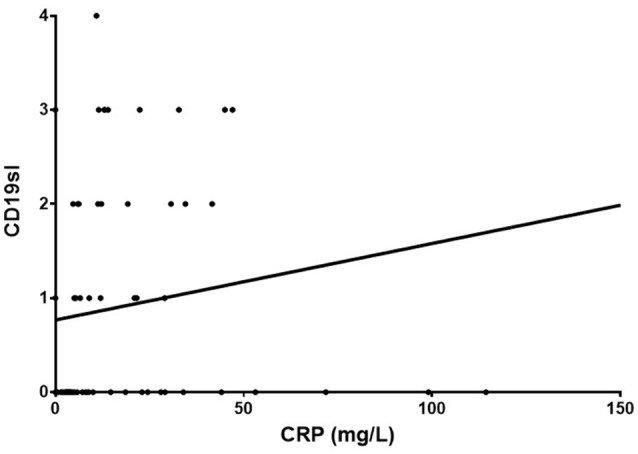
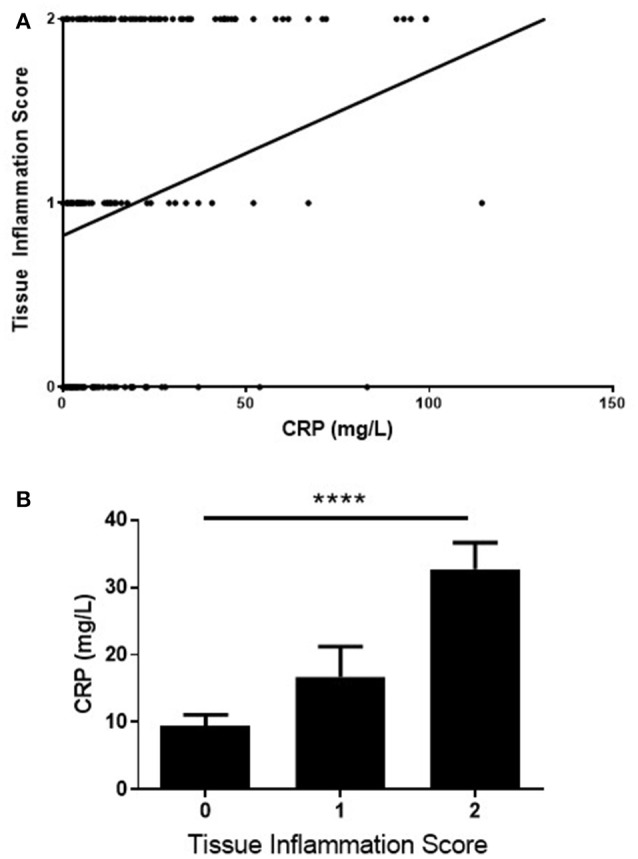
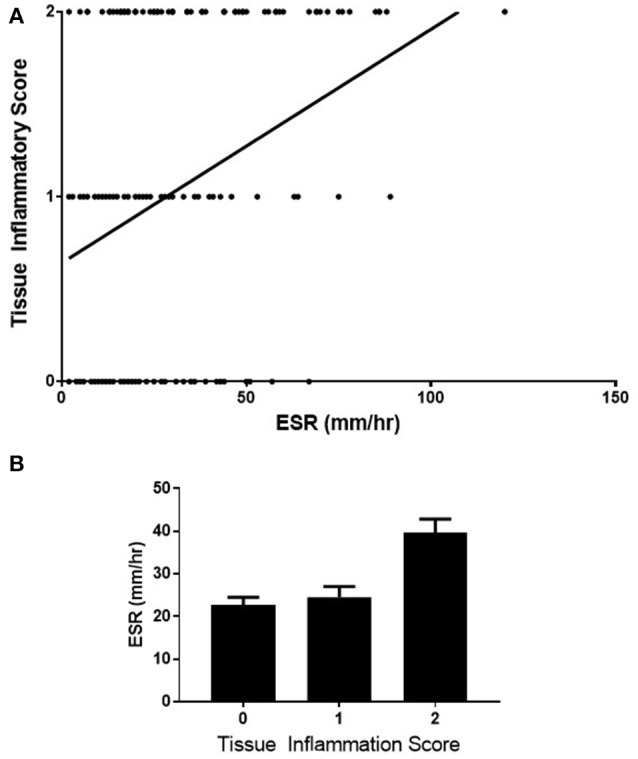
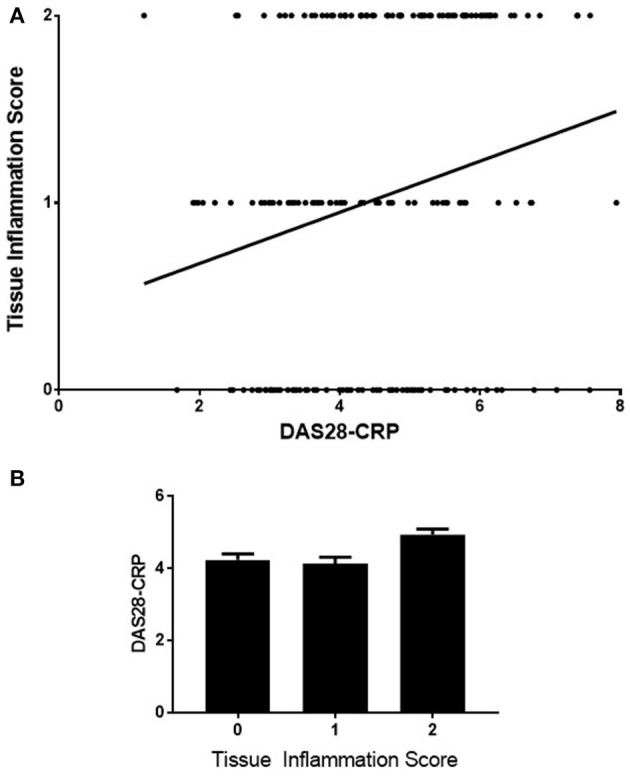
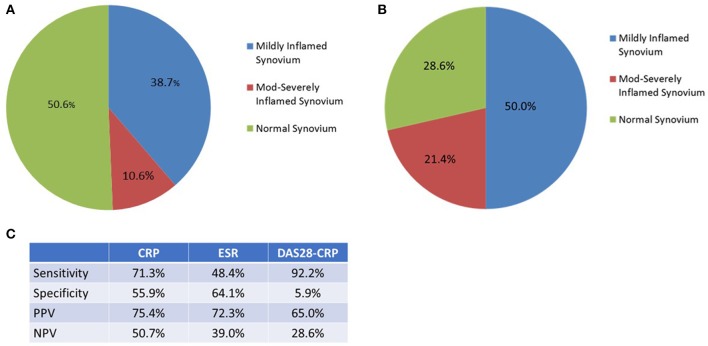
Identifying and quantifying inflammatory disease activity in rheumatoid arthritis remains a challenge. Many studies have suggested that a large proportion of patients may have active inflammation, but normal inflammatory markers. Although various disease activity scores have been validated, most rely to a large degree on biomarkers such as CRP and ESR. In this study, we examine the utility and limitations of these biomarkers, as well as the DAS28-CRP in appraising disease activity in RA. Two hundred and twenty three consecutive rheumatoid arthritis reporting knee arthralgia underwent synovial sampling of the affected knee via needle arthroscopy. The synovium was examined by microscopy with H+E staining as well as immunohistochemistry, and related to the ESR, CRP and DAS28-CRP on blood samples taken immediately before arthroscopy. Although a statistically significant positive correlation was observed between CRP and the level of inflammation in the biopsy retrieved ( = 197, rho = 0.43, CI 0.30-0.54, < 0.0001), there was histological evidence of inflammation in the synovium in 49.4% of the patients who had a normal CRP. A positive correlation was also observed between ESR and the level of inflammation in the biopsy retrieved ( = 188, rho = 0.29, CI 0.15-0.42 < 0.0001). A statistically significant but weak positive correlation was observed between the DAS28-CRP and synovial inflammation ( = 189, rho = 0.23, CI 0.09-0.37, = 0.0011). Only the CD19 infiltrate in the synovium correlated with serum CRP ( = 70, rho = 0.32, CI 0.08-0.52, = 0.0068). CRP has a moderately strong relationship with disease activity, but there are significant pitfalls in the use of this biomarker in RA, and therefore a need interpret CRP results judiciously. The results of this study underline the heterogeneity of RA, and the need to develop improved panels of biomarkers, to better stratify RA, and to identify the cohort for whom inflammatory activity cannot be measured accurately with CRP.
识别和量化类风湿性关节炎中的炎症性疾病活动仍然是一项挑战。许多研究表明,很大一部分患者可能存在活动性炎症,但炎症标志物却正常。尽管各种疾病活动评分已得到验证,但大多数在很大程度上依赖于如CRP和ESR等生物标志物。在本研究中,我们检验了这些生物标志物以及DAS28-CRP在评估类风湿性关节炎疾病活动中的效用和局限性。223例连续报告膝关节疼痛的类风湿性关节炎患者通过针式关节镜对患侧膝关节进行滑膜取样。滑膜通过苏木精-伊红(H+E)染色以及免疫组织化学进行显微镜检查,并与关节镜检查前即刻采集的血样中的ESR、CRP和DAS28-CRP相关联。尽管在CRP与活检组织中炎症水平之间观察到统计学上显著的正相关(n = 197,rho = 0.43,CI 0.30 - 0.54,P < 0.0001),但在CRP正常的患者中,有49.4%的患者滑膜存在炎症的组织学证据。在ESR与活检组织中炎症水平之间也观察到正相关(n = 188,rho = 0.29,CI 0.15 - 0.42,P < 0.0001)。在DAS28-CRP与滑膜炎症之间观察到统计学上显著但较弱的正相关(n = 189,rho = 0.23,CI 0.09 - 0.37,P = 0.0011)。滑膜中只有CD19浸润与血清CRP相关(n = 70,rho = 0.32,CI 0.08 - 0.52,P = 0.0068)。CRP与疾病活动有中度强相关性,但在类风湿性关节炎中使用该生物标志物存在重大缺陷,因此需要审慎解读CRP结果。本研究结果强调了类风湿性关节炎的异质性,以及开发改进的生物标志物组合以更好地对类风湿性关节炎进行分层并识别出无法用CRP准确测量炎症活动的队列的必要性。