Titzler Ingrid, Saruhanjan Karina, Berking Matthias, Riper Heleen, Ebert David Daniel
Friedrich-Alexander University Erlangen-Nürnberg, Institute of Psychology, Department of Clinical Psychology and Psychotherapy, Erlangen, Germany.
VU University Amsterdam, Faculty of Behavioral and Movement Sciences, Section of Clinical Psychology, Amsterdam, Netherlands.
Internet Interv. 2018 Jan 16;12:150-164. doi: 10.1016/j.invent.2018.01.002. eCollection 2018 Jun.
Blended therapies (BT) combine face-to-face (f2f) sessions with internet- and mobile-based interventions (IMIs). However, the use of blended interventions in routine care is still rare and depends on the acceptance of key health care professionals such as the therapists. Little is yet known about the therapists' perspective on and experiences with blended approaches. The aim of this pilot study was to identify barriers and facilitators, as perceived by psychotherapists, for implementing a blended therapy for depression.
Semi-structured expert interviews were conducted with five therapists, who were part of the German study arm of the FP7-project E-Compared (www.e-compared.eu). All patients ( = 173) were treated in the context of a registered RCT (DRKS00006866) in which the clinical and cost-effectiveness of BT for depression, consisting of ten internet- and mobile-based cognitive behavioral therapy modules and six f2f sessions, was compared to the treatment usually provided by general practitioners. To identify barriers and facilitators an interview guide based on the theoretical domains framework (TDF) was developed. The interviews were audio-recorded, transcribed verbatim and analyzed using a qualitative content analysis by two independent coders.
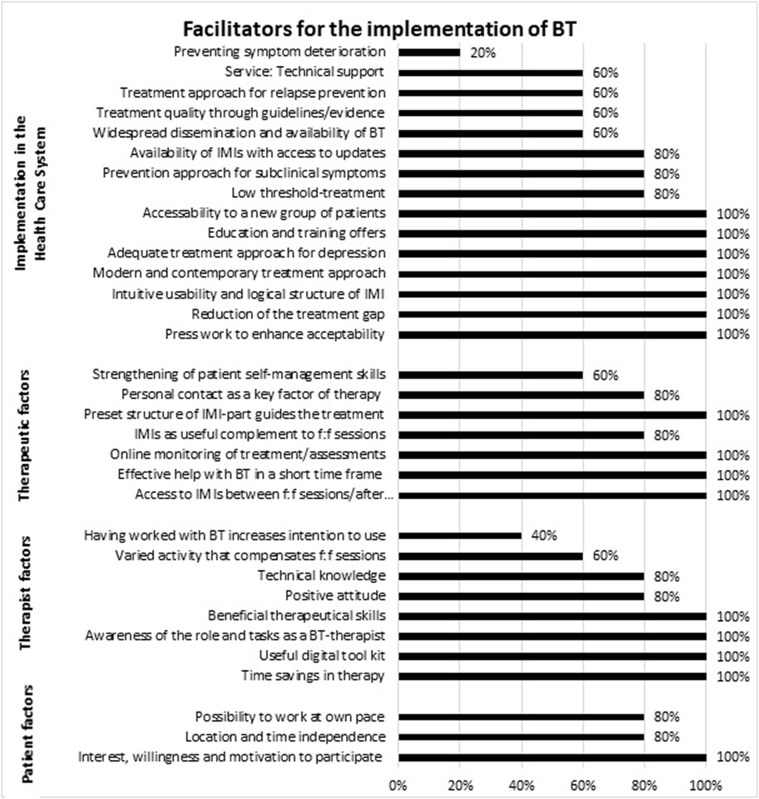
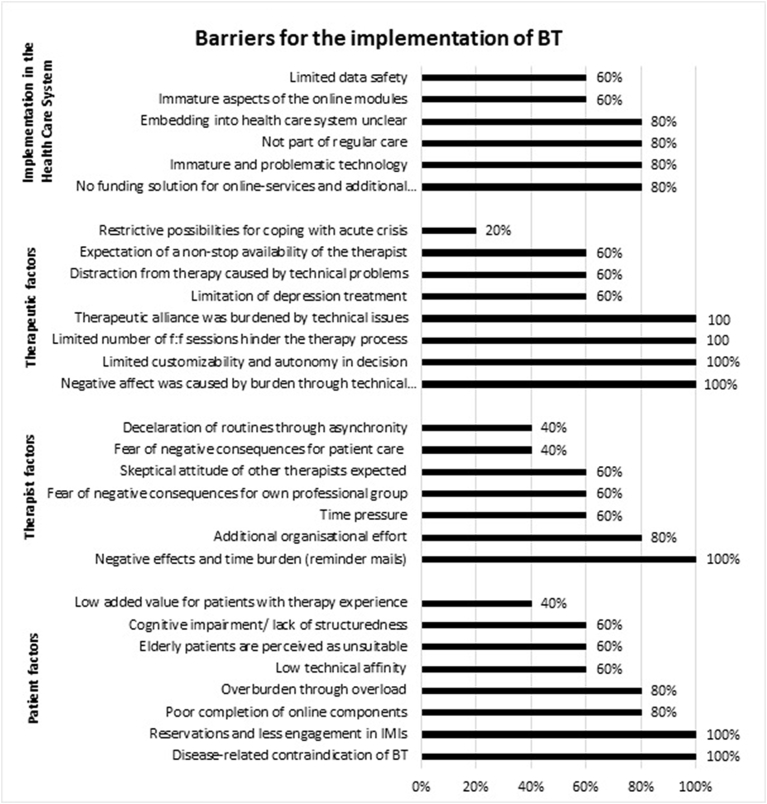
The results revealed 29 barriers and 33 facilitators, which are hindering or enabling factors on the levels of 'implementation in the health care system', 'therapy', 'therapists' and 'patients'. Key barriers stated by all therapists were 'Limited customizability and autonomy of decisions concerning blending the therapy' (number of statements, = 44); 'Disease-related contraindications for BT' ( = 25); 'Negative affect was caused by burden through technical problems' ( = 18); 'Limited number of f2f sessions hindered the therapy process'; and 'Establishment of therapeutic alliance was burdened by technical issues' (each = 15). Key facilitators stated by all therapists were: 'Patients' interest, willingness and motivation to participate' ( = 22); 'Patients' access to online content between f2f sessions and after therapy end' ( = 20); 'Preset structure of IMI-part guided the treatment course of BT' ( = 18); and 'Effective help with BT in a short time frame' ( = 15), as well as 'Reduction of the treatment gap' ( = 13).
Therapists supported the implementation of BT for depression. Results indicated the consideration of a wide range of determinants: among others, the possibility of individualizing the treatment; the autonomy of decision making in respect to the ratio and number of online and f2f sessions; the necessity of providing training; the need to develop a concept of embedding BT in the health care system and funding the additional effort; and the use of sophisticated technical solutions.
混合疗法(BT)将面对面(f2f)治疗与基于互联网和移动设备的干预措施(IMIs)相结合。然而,混合干预措施在常规护理中的应用仍然很少,并且取决于治疗师等关键医疗保健专业人员的接受程度。关于治疗师对混合疗法的看法和经验,目前所知甚少。这项试点研究的目的是确定心理治疗师认为实施抑郁症混合疗法的障碍和促进因素。
对五名治疗师进行了半结构化专家访谈,他们是FP7项目E-Compared(www.e-compared.eu)德国研究组的成员。所有患者(n = 173)均在一项注册随机对照试验(DRKS00006866)的背景下接受治疗,该试验将由十个基于互联网和移动设备的认知行为治疗模块以及六个面对面治疗课程组成的抑郁症混合疗法的临床和成本效益与全科医生通常提供的治疗进行了比较。为了确定障碍和促进因素,制定了一份基于理论领域框架(TDF)的访谈指南。访谈进行了录音,逐字转录,并由两名独立编码员使用定性内容分析法进行分析。
结果揭示了29个障碍和33个促进因素,它们是在“医疗保健系统中的实施”、“治疗”、“治疗师”和“患者”层面上的阻碍或促成因素。所有治疗师提到的关键障碍包括:“混合疗法决策的可定制性和自主性有限”(陈述数量,n = 44);“抑郁症混合疗法的疾病相关禁忌症”(n = 25);“技术问题导致的负担产生负面影响”(n = 18);“面对面治疗课程数量有限阻碍了治疗过程”;以及“技术问题给治疗联盟的建立带来负担”(各n = 15)。所有治疗师提到的关键促进因素包括:“患者参与的兴趣、意愿和动机”(n = 22);“患者在面对面治疗课程之间以及治疗结束后访问在线内容的机会”(n = 20);“IMI部分的预设结构指导了混合疗法的治疗过程”(n = 18);“在短时间内为混合疗法提供有效帮助”(n = 15),以及“缩小治疗差距”(n = 13)。
治疗师支持实施抑郁症混合疗法。结果表明需要考虑广泛的决定因素:其中包括治疗个性化的可能性;关于在线和面对面治疗课程的比例和数量的决策自主性;提供培训的必要性;制定将混合疗法纳入医疗保健系统并为额外工作提供资金的概念的必要性;以及使用先进的技术解决方案。