Medical Sociology Unit, Hannover Medical School, Hannover, Germany.
Local Statutory Health Insurance of Lower Saxony (AOK Niedersachsen), Hannover, Germany.
PLoS One. 2018 Aug 23;13(8):e0202631. doi: 10.1371/journal.pone.0202631. eCollection 2018.
According to James Fries morbidity compression is present if morbidity rates are decreasing to a larger extent than mortality rates. Compression also occurs if age at onset is increasing at a faster pace than age at death. These two variants of the compression hypothesis were formulated as a population concept. Compression has seldom been studied with a specific disease as application.
Morbidity compression was examined in terms of myocardial infarction (MI) by using German claims data covering the years 2006 to 2015. The findings are based on an annual case number of about 2 m women and men aged 18 years and older. Analyses were performed by means of proportional hazards regression and by using linear regression.
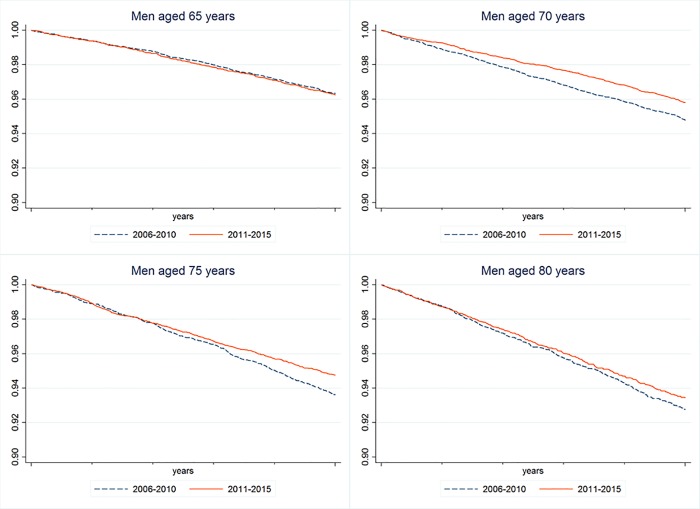
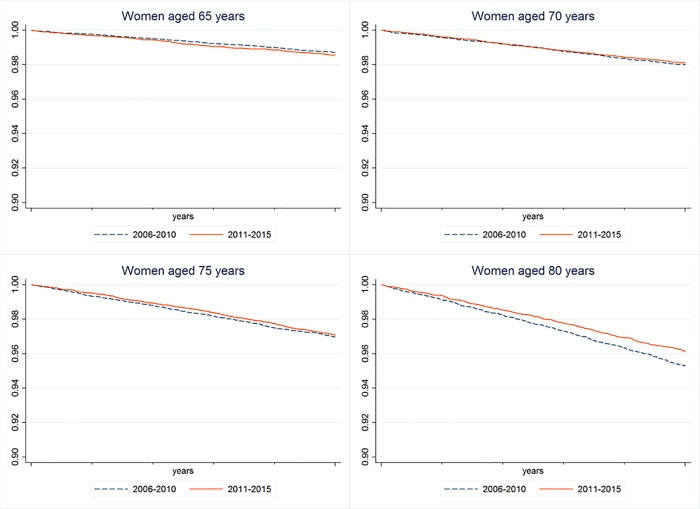
Decreases of morbidity rates were more pronounced than those of mortality. For men, the hazard ratio for contracting MI in 2015 as compared to 2006 was hr = 0.66 and hr = 0.71 for the female population. The respective results for mortality were hr = 0.75 in men and hr = 1.0 in women. They can be interpreted in favor of morbidity compression. For the subgroup of women and men with MI, changes of onset age revealed marked gender differences. For 2015 as compared with 2006, age at MI-occurrence in men increased by 10.5 months as compared to an increase of 10.4 months for age at death. In women changes were smaller and statistically not significant. The findings referring to women have to be interpreted against the backdrop of higher onset age and higher age at death than in men.
Taken together, morbidity compression has occurred in terms of decreasing MI-rates as well as in terms of increased onset age in men. It can be concluded that both processes have led to an improvement of healthy lifetime. Decreasing morbidity rates in women are also pointing towards morbidity compression, a finding that is not complemented by changes of onset age. Our data are demonstrating that morbidity rates and age at onset may vary independently. From this perspective morbidity compression is a multi-faceted phenomenon.
根据詹姆斯·弗里斯(James Fries)的说法,如果发病率的下降幅度大于死亡率,那么发病率就会出现压缩。如果发病年龄的增长速度快于死亡年龄,也会出现这种情况。这两种发病率压缩假说的变体都是作为人口概念提出的。很少有研究以特定疾病为应用来研究发病率压缩。
利用德国索赔数据,对 2006 年至 2015 年期间的心肌梗死(MI)发病率进行了压缩研究。这些发现是基于每年约 200 万 18 岁及以上的女性和男性的病例数。通过比例风险回归和线性回归进行分析。
发病率的下降幅度大于死亡率的下降幅度。对于男性,与 2006 年相比,2015 年患 MI 的风险比为 HR = 0.66,女性为 HR = 0.71。死亡率的相应结果为男性 HR = 0.75,女性 HR = 1.0。这可以解释为发病率压缩。对于患有 MI 的女性和男性亚组,发病年龄的变化显示出明显的性别差异。与 2006 年相比,2015 年男性 MI 发病年龄增加了 10.5 个月,而死亡年龄增加了 10.4 个月。女性的变化较小,且无统计学意义。考虑到女性的发病年龄和死亡年龄高于男性,因此对于女性的发现必须加以解释。
总的来说,男性的 MI 发病率下降和发病年龄增加都出现了发病率压缩。可以得出结论,这两个过程都导致了健康寿命的延长。女性发病率的下降也表明发病率压缩,而发病年龄的变化则没有补充这一发现。我们的数据表明,发病率和发病年龄可能会独立变化。从这个角度来看,发病率压缩是一个多方面的现象。