Mori Sotaro, Kurimoto Takuji, Ueda Kaori, Enomoto Hiroko, Sakamoto Mari, Keshi Yukako, Yamada Yuko, Nakamura Makoto
Division of Ophthalmology, Department of Surgery, Kobe University Graduate School of Medicine, Kobe, Japan.
Case Rep Ophthalmol. 2018 Jul 20;9(2):348-356. doi: 10.1159/000491075. eCollection 2018 May-Aug.
Recent immune therapy with checkpoint inhibitors (CPIs) has demonstrated remarkable antitumor effects on specific tumors, such as malignant lymphoma and non-small cell lung carcinoma. By contrast, CPIs cause an imbalance in the immune system, triggering a wide range of immunological side effects termed immune-related adverse effects (irAEs). Here, we report a rare case of optic neuritis and hypopituitarism during anti-programmed death-ligand 1 (PD-L1) antibody treatment.
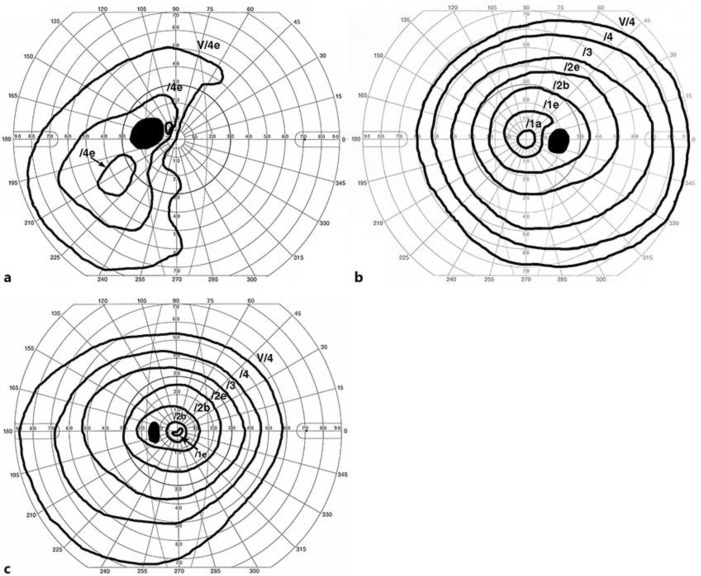
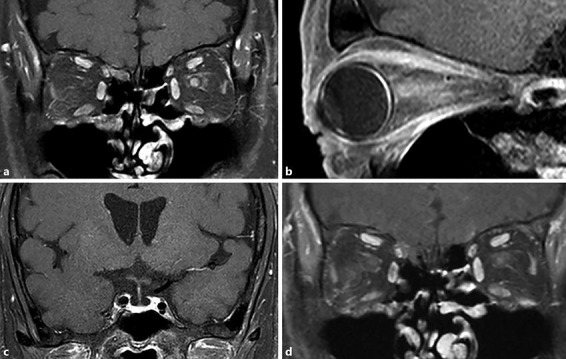
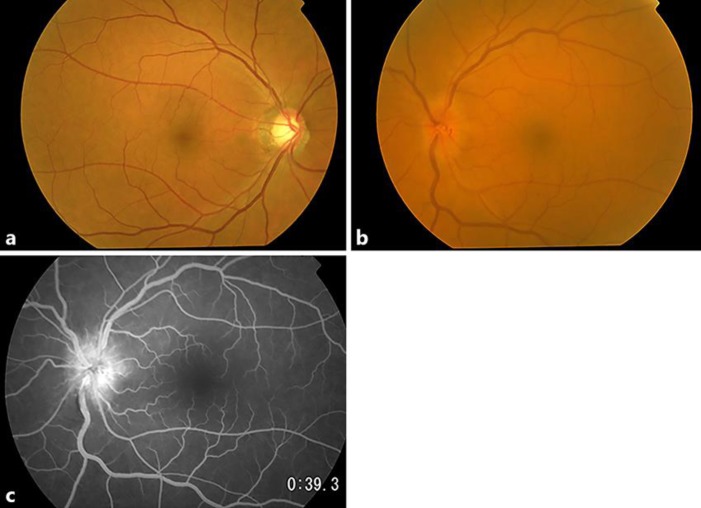
A patient with non-small cell lung carcinoma received anti-PD-L1 antibody treatment every 3 weeks; however, the patient started experiencing headaches, general fatigue, anorexia, and diarrhea approximately 1 year after the initiation of the treatment. Moreover, sudden visual loss of the right eye occurred 1 week after the interruption of the anti-PD-L1 antibody treatment. MRI findings showed gadolinium enhancement in the left optic nerve, but no enlargement of the pituitary gland and stalk. Laboratory data showed decreased serum adrenocorticotropic hormone (ACTH), cortisol, and free T levels, and a hormone tolerance test indicated hypopituitarism, hypothyroidism, and hypoadrenocorticism. The central scotoma caused by optic neuritis completely disappeared immediately after a course of steroid pulse therapy, and no recurrence occurred up to 2 years after initiation of the steroid pulse therapy while replacement therapy for hypothyroidism and hypoadrenocorticism was continued.
The patient presented with optic neuritis and hypopituitarism, possibly due to irAEs of the anti-PD-L1 antibody treatment. Steroid pulse therapy was effective for optic neuritis, suggesting underlying immunological mechanisms. Neurological complications including optic neuritis should be considered when examining patients with cancer undergoing CPI treatment.
近期使用检查点抑制剂(CPI)的免疫疗法已在特定肿瘤(如恶性淋巴瘤和非小细胞肺癌)上显示出显著的抗肿瘤效果。相比之下,CPI会导致免疫系统失衡,引发一系列称为免疫相关不良反应(irAE)的免疫副作用。在此,我们报告一例在抗程序性死亡配体1(PD-L1)抗体治疗期间发生视神经炎和垂体功能减退的罕见病例。
一名非小细胞肺癌患者每3周接受一次抗PD-L1抗体治疗;然而,在治疗开始约1年后,患者开始出现头痛、全身乏力、厌食和腹泻。此外,在抗PD-L1抗体治疗中断1周后,右眼突然失明。MRI检查结果显示左侧视神经钆增强,但垂体和垂体柄无增大。实验室数据显示血清促肾上腺皮质激素(ACTH)、皮质醇和游离T水平降低,激素耐量试验表明存在垂体功能减退、甲状腺功能减退和肾上腺皮质功能减退。在进行一个疗程的类固醇脉冲治疗后,由视神经炎引起的中心暗点立即完全消失,在开始类固醇脉冲治疗后2年内未复发,同时继续进行甲状腺功能减退和肾上腺皮质功能减退的替代治疗。
该患者出现视神经炎和垂体功能减退,可能是由于抗PD-L1抗体治疗的irAE所致。类固醇脉冲治疗对视神经炎有效,提示存在潜在的免疫机制。在检查接受CPI治疗的癌症患者时,应考虑包括视神经炎在内的神经系统并发症。