Tienza Antonio, Akin Yigit, Rassweiler Jens, Gözen Ali Serdar
Department of Urology, Clinica Universidad de Navarra, Pamplona, Spain.
Department of Urology, Harran University School of Medicine, Yenisehir Campus, Sanliurfa, Turkey.
Prostate Int. 2018 Sep;6(3):94-98. doi: 10.1016/j.prnil.2017.09.001. Epub 2017 Sep 24.
We aimed to study the continence between intermediate and high-risk cancer patients and the influential factors to recover continence.
In total, 655 patients underwent surgery by robot-assisted radical prostatectomy between 2010 and 2015. Of 655 patients, 294 were classified according to D'Amico risk groups as intermediate risk or high risk and completed the micturition protocol. Patients with intermediate risk were matched in a 1:1 ratio to patients with high risk for age and body mass index. Urine loss ratio (ULR) was defined as urine loss divided by micturition volumes. Immediate continence was defined with the best cut-off value of ULR.
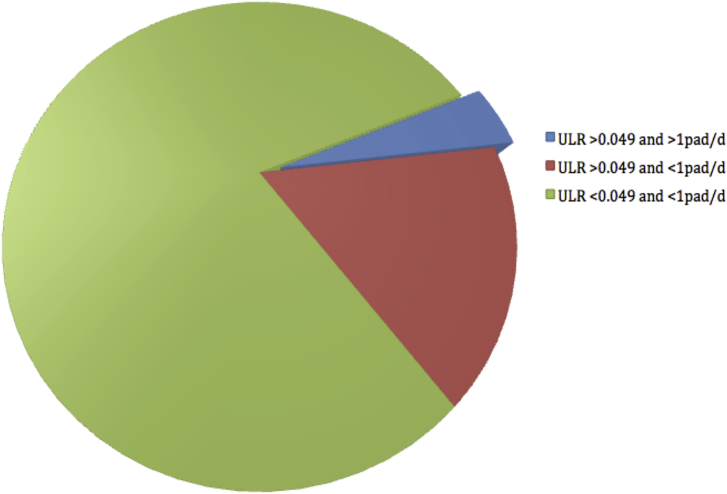
In total, 117 patients with intermediate risk were matched to those with high risk. The comparison did not show any statistically significant difference in the ULR value ( = 0.359) or continence rate ( = 0.449). Predictive analysis was performed for the 294 patients (intermediate and high risk), of which 9.5% were classified as incontinent (>1 pad/d). Immediate continence was defined as ULR < 0.049 in 232 (78.9%) patients. Age, preoperative hemoglobin, and duration of catheterization were found influent by univariate analysis. Only age [odds ratio (OR) = 1.072; 95% confidence interval (CI) = 1.020-1.127; = 0.006] and duration of catheterization (OR = 1.060; 95% CI = 1.003-1.120; = 0.040) were independent influential factors to predict immediate continence.
D'Amico intermediate- and high-risk groups do not differ in continence terms. The ULR value of < 0.049 identifies those patients who recover continence earlier. Age and duration of catheterization were influential factors in predicting immediate continence.
我们旨在研究中高危癌症患者的控尿情况以及影响控尿恢复的因素。
2010年至2015年间,共有655例患者接受了机器人辅助根治性前列腺切除术。在这655例患者中,294例根据达米科风险分组被归类为中危或高危,并完成了排尿方案。中危患者与高危患者按年龄和体重指数1:1的比例进行匹配。尿失禁率(ULR)定义为尿失禁量除以排尿量。根据ULR的最佳临界值定义即刻控尿。
总共117例中危患者与高危患者进行了匹配。比较结果显示,ULR值(P = 0.359)或控尿率(P = 0.449)在统计学上没有显著差异。对294例患者(中危和高危)进行了预测分析,其中9.5%被归类为尿失禁(>1片/天)。232例(78.9%)患者的即刻控尿定义为ULR < 0.049。单因素分析发现年龄、术前血红蛋白和导尿持续时间有影响。只有年龄[比值比(OR)= 1.072;95%置信区间(CI)= 1.020 - 1.127;P = 0.006]和导尿持续时间(OR = 1.060;95% CI = 1.003 - 1.120;P = 0.040)是预测即刻控尿的独立影响因素。
达米科中高危组在控尿方面没有差异。ULR值< 0.049可识别出那些较早恢复控尿的患者。年龄和导尿持续时间是预测即刻控尿的影响因素。