Bauernfreund Yehudit, Butler Matthew, Ragavan Sumathi, Sampson Elizabeth L
North Middlesex Hospital, London, UK.
Care of the Elderly Department, North Middlesex Hospital, London, UK.
BMJ Open Qual. 2018 Aug 13;7(3):e000200. doi: 10.1136/bmjoq-2017-000200. eCollection 2018.
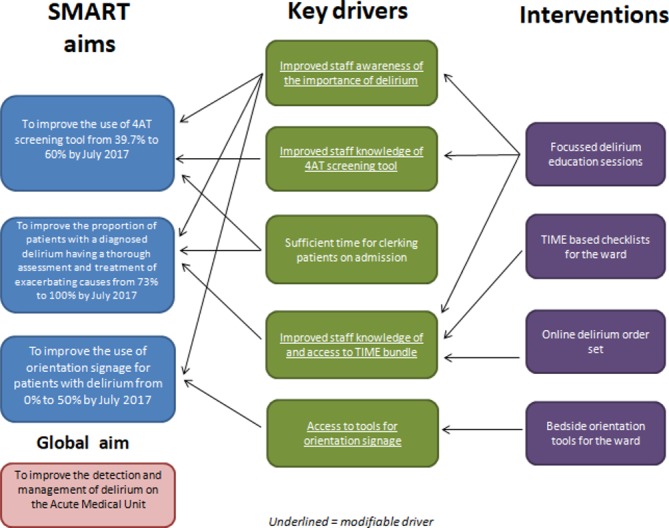
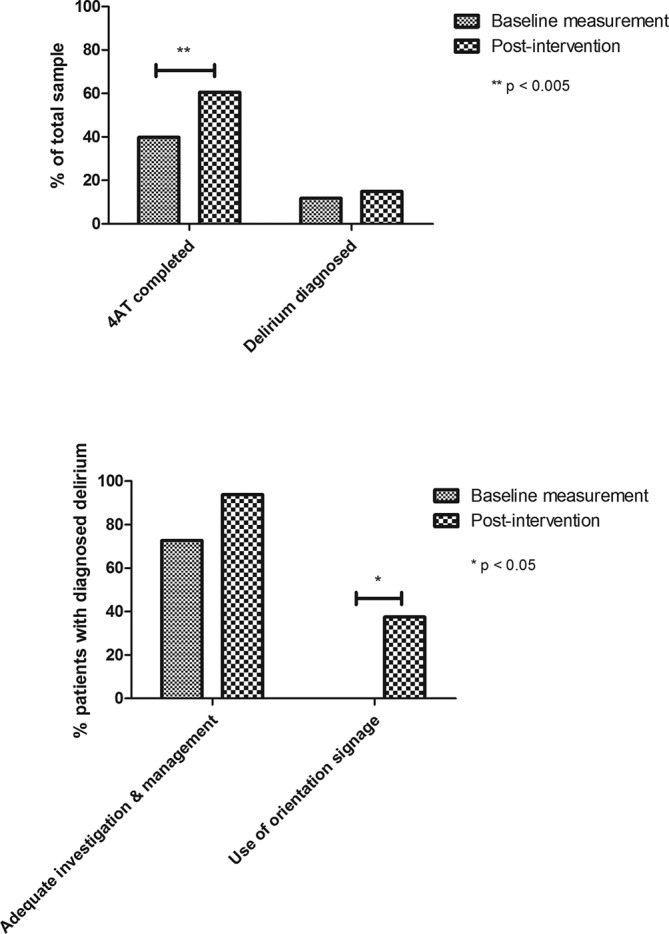
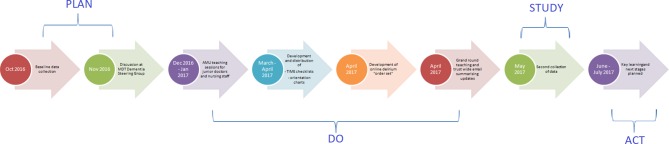
Delirium affects 18%-35% patients in the acute hospital setting, yet is often neither detected nor managed appropriately. It is associated with increased risk of falls, longer hospital stay and increased morbidity and mortality rates. It is a frightening and unpleasant experience for both patients and their families. We used quality improvement tools and a multicomponent intervention to promote detection and improve management of delirium on the acute medical unit (AMU). We reviewed whether a delirium screening tool (4AT) had been completed for all patients aged over 65 years admitted to the AMU over 1 week. If delirium was detected, we assessed whether investigation and management was adequate as per national guidance. After baseline data collection, we delivered focused sessions of delirium education for doctors and nursing staff, including training on use of the 4AT tool and the TIME (Triggers, Investigate, Manage, Engage) management bundle. We introduced TIME checklists, an online delirium order set and created a bedside orientation tool. We collected data following the interventions and identified areas for further improvement. Following our first PDSA (Plan, Do, Study, Act) cycle, use of the 4AT screening tool improved from 40% to 61%. Adequate assessment for the causes of and exacerbating factors for delirium increased from 73% to 94% of cases. Use of personal orientation tools improved from 0% to 38%. In summary, a targeted staff education programme and practical aids for the ward have improved the screening and management of delirium on the AMU. This may be improved further through more frequent training sessions to account for regular change-over of junior doctors and through implementing a nursing champion for delirium.
在急性医院环境中,谵妄影响18%-35%的患者,但往往未被及时发现,也未得到妥善处理。它与跌倒风险增加、住院时间延长以及发病率和死亡率上升有关。这对患者及其家属来说都是可怕且不愉快的经历。我们运用质量改进工具和多组分干预措施,以促进对急性内科病房(AMU)谵妄的检测并改善其管理。我们回顾了在1周内入住AMU的所有65岁以上患者是否完成了谵妄筛查工具(4AT)。如果检测到谵妄,我们会根据国家指南评估调查和管理是否充分。在收集基线数据后,我们为医生和护理人员开展了谵妄教育重点课程,包括4AT工具及TIME(触发因素、调查、管理、参与)管理包的使用培训。我们引入了TIME检查表、在线谵妄医嘱集,并创建了床边定向工具。我们在干预后收集数据,并确定需要进一步改进的领域。在我们的第一个PDSA(计划、执行、研究、行动)循环之后,4AT筛查工具的使用率从40%提高到了61%。对谵妄病因和加重因素的充分评估从73%的病例增加到了94%。个人定向工具的使用率从0%提高到了38%。总之,针对病房工作人员的定向教育计划和实用辅助工具改善了AMU对谵妄的筛查和管理。通过更频繁的培训课程以适应初级医生的定期轮换,并通过设立一名谵妄护理负责人,这一情况可能会得到进一步改善。