Division of Otolaryngology - Head and Neck Surgery, Western University and London Health Sciences Centre, 5010, 800 Commissioners Road E, London, Ontario, Canada.
Division of Otolaryngology - Head and Neck Surgery, University of British Columbia, Vancouver, BC, Canada.
J Otolaryngol Head Neck Surg. 2018 Sep 3;47(1):52. doi: 10.1186/s40463-018-0297-4.
Patients with vestibular schwannomas (VS) are faced with complex management decisions. Watchful waiting, surgical resection, and radiation are all viable options with associated risks and benefits. We sought to determine if patients with VS experience decisional conflict when deciding between surgery or non-surgical management, and factors influencing the degree of decisional conflict.
A prospective cohort study in two tertiary ambulatory skull-base clinics was performed. Patients with newly diagnosed or newly growing vestibular schwannomas were recruited. Patients were given a demographic form and the decisional conflict scale (DCS), a validated measure to assess the degree of uncertainty when making medical decisions. The degree of shared decision making (SDM) experienced by the patient and physician were assessed via the SDM-Q-10 and SDM-Q-Doc questionnaires, respectively. Non-parametric statistics were used. Questionnaires and demographic information were correlated with DCS using Spearman correlation coefficient and Mann-Whitney U. Logistic regression was performed to determine factors independently associated with DCS scores.
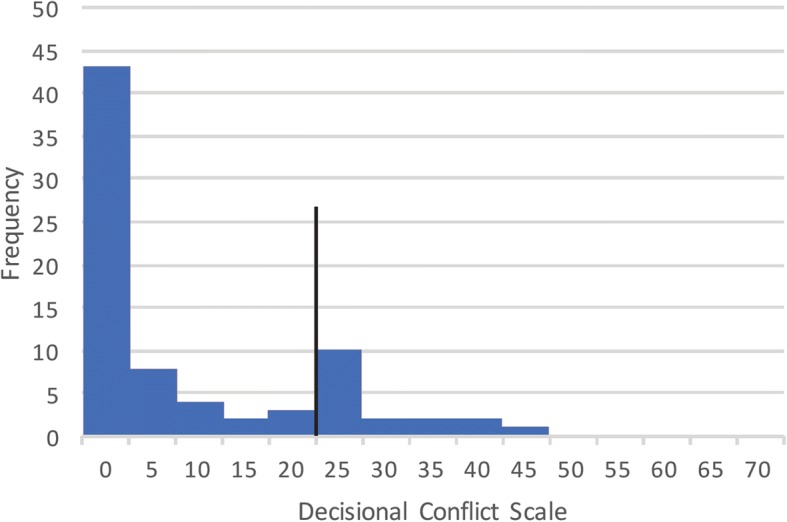
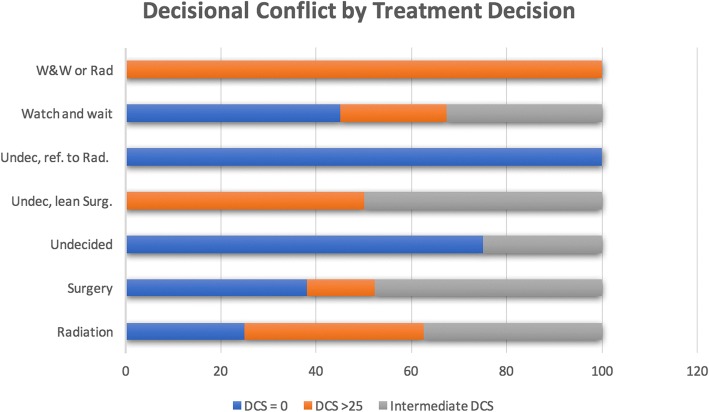
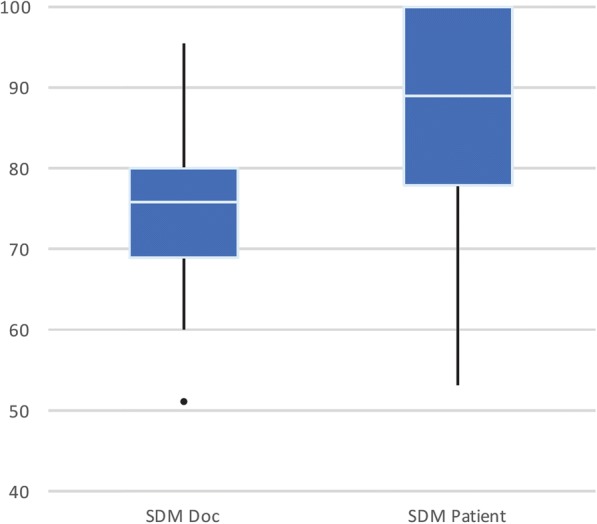
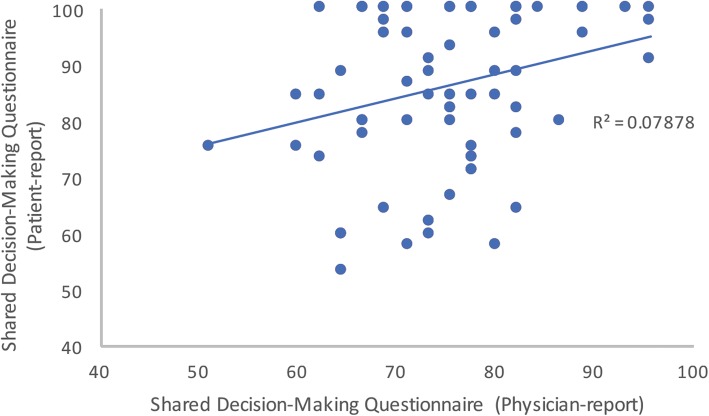
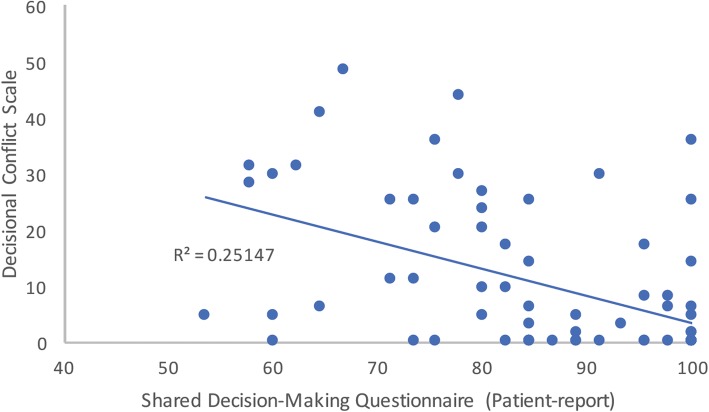
Seventy-seven patients participated (55% female, aged 37-81 years); VS ranged in size from 2 mm-50 mm. Significant decisional conflict (DCS score 25 or greater) was experienced by 17 (22%) patients. Patients reported an average SDM-Q-10 score of 86, indicating highly perceived level of SDM. Physician and patient SDM scores were weakly correlated (p = 0.045, Spearman correlation coefficient 0.234). DCS scores were significantly negatively correlated with a decision to pursue surgery, presence of a trainee, and higher SDM-Q-10 score. DCS was higher with female gender. Using logistic regression, the SDM-Q-10 score was the only variable associated with significantly reduced DCS.
About one fifth of patients deciding how to manage their vestibular schwannoma experienced a significant degree of decisional conflict. Involving the patients in the process through shared decision-making significantly reduced the degree of uncertainty patients experienced.
前庭神经鞘瘤(VS)患者面临着复杂的管理决策。观察等待、手术切除和放疗都是可行的选择,各有其风险和益处。我们旨在确定 VS 患者在选择手术或非手术治疗时是否会经历决策冲突,以及影响决策冲突程度的因素。
在两家三级门诊颅底诊所进行前瞻性队列研究。招募新诊断或新增大的前庭神经鞘瘤患者。患者填写一份人口统计学表格和决策冲突量表(DCS),这是一种评估在做出医疗决策时不确定性程度的有效衡量标准。通过决策参与量表(SDM-Q-10)和决策支持医师量表(SDM-Q-Doc)分别评估患者和医生的决策共享程度。采用非参数统计方法。使用 Spearman 相关系数和 Mann-Whitney U 检验将问卷和人口统计学信息与 DCS 进行相关分析。进行逻辑回归以确定与 DCS 评分独立相关的因素。
77 名患者参与(55%为女性,年龄 37-81 岁);VS 大小从 2 毫米到 50 毫米不等。17 名(22%)患者经历了显著的决策冲突(DCS 评分 25 或更高)。患者报告的平均决策参与量表(SDM-Q-10)得分为 86,表明他们高度感知到决策共享程度。医生和患者的决策共享评分呈弱相关(p=0.045,Spearman 相关系数 0.234)。DCS 评分与手术治疗决策、有培训生参与以及更高的 SDM-Q-10 评分显著负相关。女性患者的 DCS 评分更高。使用逻辑回归,SDM-Q-10 评分是唯一与 DCS 显著降低相关的变量。
约五分之一决定如何管理前庭神经鞘瘤的患者经历了显著程度的决策冲突。通过决策共享让患者参与其中,显著降低了患者的不确定性程度。