Vascular Research Group, Department of Renal Medicine, Salford Royal NHS Foundation Trust, Stott Lane, Salford, M6 8HD, UK.
Faculty of Biology, Medicine and Health, University of Manchester, Manchester, UK.
J Nephrol. 2018 Dec;31(6):931-939. doi: 10.1007/s40620-018-0529-8. Epub 2018 Sep 5.
In older patients with chronic kidney disease (CKD), the risk of progression to end stage renal disease and cardiovascular death both differ compared to younger patients. This likely reflects differences in case mix and co-morbid burdens. We sought to establish the extent to which age itself is an independent biomarker of adverse outcome in CKD.
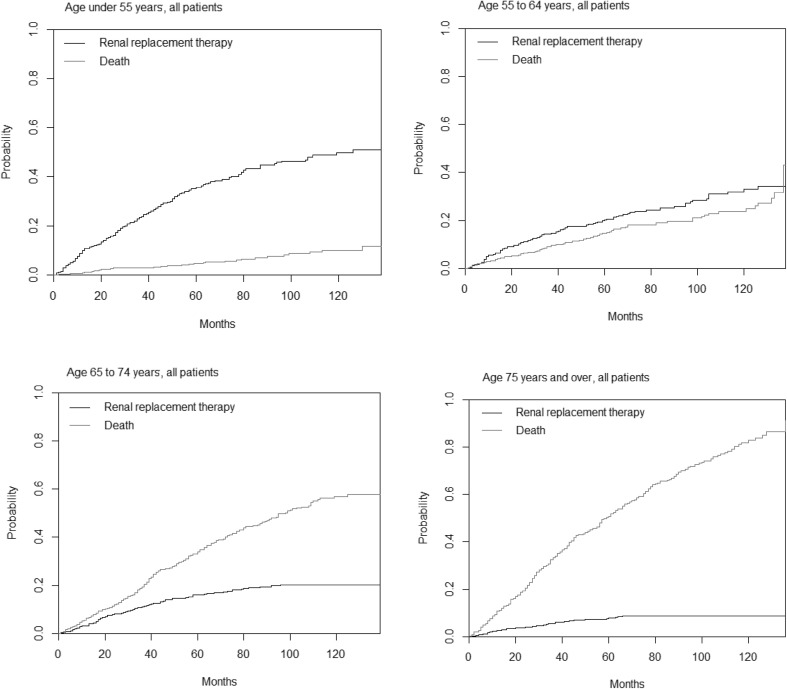
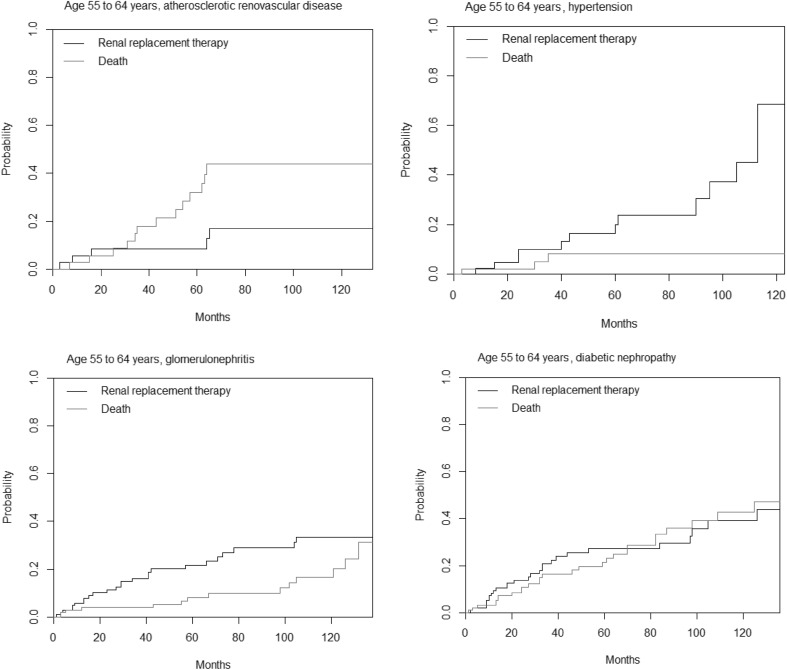
This was an analysis of the Salford Kidney Study, a prospective, longitudinal, observational study of 2,667 patients with eGFR < 60 ml/min/1.73 m. Patients were divided into four age groups (< 55, 55-65, 65-75 and > 75 years). Within group adjusted hazard ratios for death in older compared to younger patients were calculated for different primary renal diseases. A competing risk model of death and renal replacement therapy (RRT) as outcomes was performed.
The median age of the cohort was 67.1 years [interquartile range (IQR): 55.6-75.3] and median eGFR 30.8 ml/min/1.73 m (IQR: 20.6-43.2). Follow up was 3.5 ± 2.9 years. Overall, the adjusted HR for death in patients aged > 75 years compared to those < 55 years was 4.4 (95% CI 3.4-5.9), p < 0.001. The HR for death differed between primary renal diseases and CKD stages. In diabetic nephropathy, the HR was 3.0 (1.8-5.3, p < 0.001), in glomerulonephritis the HR was 12.2 (5.6-25.5, p < 0.001). The cumulative incidence of RRT was < 0.1 at 10 years for patients > 75 years, compared with 0.50 in those < 55 years. Death was more likely at 20 months in those aged 75 years or older (0.17) than at 10 years in those aged < 55 years (0.10).
This study demonstrates that the risk associated with older age shows significant variability between primary renal diseases. This is whilst acknowledging that observational studies carry the risk of hidden bias not adjusted for in the statistical model.
在患有慢性肾脏病(CKD)的老年患者中,进展为终末期肾病和心血管死亡的风险均与年轻患者不同。这可能反映了病例组合和合并症负担的差异。我们试图确定年龄本身在 CKD 不良结局中的程度是否为独立的生物标志物。
这是对 Salford Kidney 研究的分析,这是一项对 2667 名 eGFR<60ml/min/1.73m 的患者进行的前瞻性、纵向、观察性研究。患者被分为四组年龄组(<55 岁、55-65 岁、65-75 岁和>75 岁)。计算了年龄较大的患者与年龄较小的患者相比,不同原发性肾脏疾病死亡的组内调整后危险比。对死亡和肾脏替代治疗(RRT)作为结局的竞争风险模型进行了分析。
队列的中位年龄为 67.1 岁[四分位距(IQR):55.6-75.3],中位 eGFR 为 30.8ml/min/1.73m(IQR:20.6-43.2)。随访时间为 3.5±2.9 年。总体而言,年龄>75 岁的患者与<55 岁的患者相比,死亡的调整后 HR 为 4.4(95%CI 3.4-5.9),p<0.001。死亡风险在原发性肾脏疾病和 CKD 分期之间存在差异。在糖尿病肾病中,HR 为 3.0(1.8-5.3,p<0.001),在肾小球肾炎中,HR 为 12.2(5.6-25.5,p<0.001)。在年龄>75 岁的患者中,10 年内 RRT 的累积发生率<0.1,而在年龄<55 岁的患者中,累积发生率为 0.50。在年龄 75 岁或以上的患者中,在 20 个月时死亡的可能性(0.17)高于年龄<55 岁的患者在 10 年内(0.10)。
本研究表明,与年龄相关的风险在原发性肾脏疾病之间存在显著差异。这是在承认观察性研究存在统计学模型未调整的潜在偏倚的风险的情况下得出的。