Heuvelings Charlotte C, Greve Patrick F, de Vries Sophia G, Visser Benjamin, Bélard Sabine, Janssen Saskia, Cremers Anne L, Spijker René, Shaw Elizabeth, Hill Ruaraidh A, Zumla Alimuddin, Sandgren Andreas, van der Werf Marieke J, Grobusch Martin Peter
Department of Infectious Diseases, Division of Internal Medicine, Academic Medical Center, Center of Tropical Medicine and Travel Medicine, University of Amsterdam, Amsterdam, The Netherlands.
Medical Library, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands.
BMJ Open. 2018 Sep 8;8(9):e019642. doi: 10.1136/bmjopen-2017-019642.
To determine which service models and organisational structures are effective and cost-effective for delivering tuberculosis (TB) services to hard-to-reach populations.
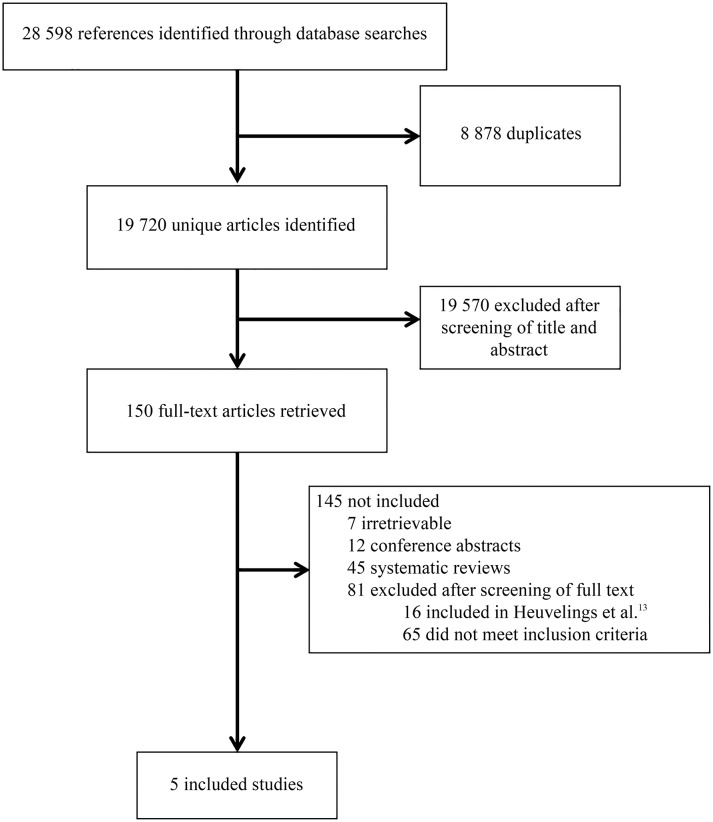
Embase and MEDLINE (1990-2017) were searched in order to update and extend the 2011 systematic review commissioned by National Institute for Health and Care Excellence (NICE), discussing interventions targeting service models and organisational structures for the identification and management of TB in hard-to-reach populations. The NICE and Cochrane Collaboration standards were followed.
European Union, European Economic Area, European Union candidate countries and Organisation for Economic Co-operation and Development countries.
Hard-to-reach populations, including migrants, homeless people, drug users, prisoners, sex workers, people living with HIV and children within vulnerable and hard-to-reach populations.
Effectiveness and cost-effectiveness of the interventions.
From the 19 720 citations found, five new studies were identified, in addition to the six discussed in the NICE review. Community health workers from the same migrant community, street teams and peers improved TB screening uptake by providing health education, promoting TB screening and organising contact tracing. Mobile TB clinics, specialised TB clinics and improved cooperation between healthcare services can be effective at identifying and treating active TB cases and are likely to be cost-effective. No difference in treatment outcome was detected when directly observed therapy was delivered at a health clinic or at a convenient location in the community.
Although evidence is limited due to the lack of high-quality studies, interventions using peers and community health workers, mobile TB services, specialised TB clinics and improved cooperation between health services can be effective to control TB in hard-to-reach populations. Future studies should evaluate the (cost-)effectiveness of interventions on TB identification and management in hard-to-reach populations and countries should be urged to publish the outcomes of their TB control systems.
CRD42015017865.
确定哪些服务模式和组织结构在为难以接触到的人群提供结核病(TB)服务方面是有效且具有成本效益的。
检索了Embase和MEDLINE(1990 - 2017年),以更新和扩展英国国家卫生与临床优化研究所(NICE)委托进行的2011年系统评价,该评价讨论了针对难以接触到的人群中结核病识别和管理的服务模式及组织结构的干预措施。遵循了NICE和Cochrane协作组的标准。
欧盟、欧洲经济区、欧盟候选国家以及经济合作与发展组织国家。
难以接触到的人群,包括移民、无家可归者、吸毒者、囚犯、性工作者、艾滋病毒感染者以及弱势群体和难以接触到的人群中的儿童。
干预措施的有效性和成本效益。
在检索到的19720篇文献中,除了NICE评价中讨论的6项研究外,还确定了5项新研究。来自同一移民社区的社区卫生工作者、街头团队和同伴通过提供健康教育、促进结核病筛查和组织接触者追踪,提高了结核病筛查的接受率。流动结核病诊所、专门的结核病诊所以及医疗服务之间加强合作,在识别和治疗活动性结核病病例方面可能有效,并且可能具有成本效益。在诊所或社区便利地点进行直接观察治疗时,未发现治疗效果有差异。
尽管由于缺乏高质量研究,证据有限,但利用同伴和社区卫生工作者、流动结核病服务、专门的结核病诊所以及改善卫生服务之间的合作等干预措施,在控制难以接触到的人群中的结核病方面可能有效。未来的研究应评估针对难以接触到的人群中结核病识别和管理干预措施的(成本)效益,并且应敦促各国公布其结核病控制系统的成果。
PROSPERO注册号:CRD42015017865。