First Department of Medicine, University Medical Centre Mannheim (UMM), Faculty of Medicine Mannheim, University of Heidelberg, Theodor-Kutzer-Ufer 1-3, 68167, Mannheim, Germany.
European Center for AngioScience (ECAS) and DZHK (German Center for Cardiovascular Research) Partner Site Heidelberg/Mannheim, Mannheim, Germany.
Cardiovasc Diabetol. 2018 Sep 10;17(1):125. doi: 10.1186/s12933-018-0768-y.
The study sought to assess the prognostic impact of type 2 diabetes in patients presenting with ventricular tachyarrhythmias on admission.
Data regarding the prognostic outcome of diabetics presenting with ventricular tachyarrhythmias is limited.
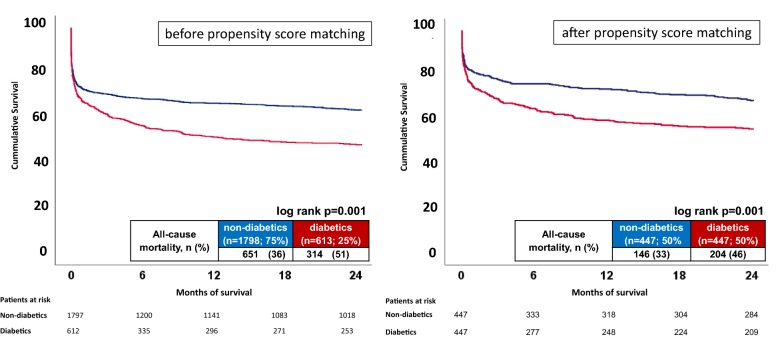
A large retrospective registry was used including all consecutive patients presenting with ventricular tachycardia (VT) and fibrillation (VF) on admission from 2002 to 2016. Patients with type 2 diabetes (diabetics) were compared to non-diabetics applying multivariable Cox regression models and propensity-score matching for evaluation of the primary prognostic endpoint of long-term all-cause mortality at 2 years. Secondary prognostic endpoints were cardiac death at 24 h, in-hospital death at index, all-cause mortality at 30 days, all-cause mortality in patients surviving index hospitalization at 2 years (i.e. "after discharge") and rehospitalization due to recurrent ventricular tachyarrhythmias at 2 years.
In 2411 unmatched high-risk patients with ventricular tachyarrhythmias, diabetes was present in 25% compared to non-diabetics (75%). Rates of VT (57% vs. 56%) and VF (43% vs. 44%) were comparable in both groups. Multivariable Cox regression models revealed diabetics associated with the primary endpoint of long-term all-cause mortality at 2 years (HR = 1.513; p = 0.001), which was still proven after propensity score matching (46% vs. 33%, log rank p = 0.001; HR = 1.525; p = 0.001). The rates of secondary endpoints were higher for in-hospital death at index, all-cause mortality at 30 days, as well as after discharge, but not for cardiac death at 24 h or rehospitalization due to recurrent ventricular tachyarrhythmias.
Presence of type 2 diabetes is independently associated with an increase of all-cause mortality in patients presenting with ventricular tachyarrhythmias on admission.
本研究旨在评估入院时伴有室性心动过速(VT)和室颤(VF)的 2 型糖尿病患者的预后影响。
目前有关糖尿病患者伴发室性心动过速的预后数据有限。
本研究使用了一个大型回顾性登记数据库,纳入了 2002 年至 2016 年期间所有因 VT 和 VF 入院的连续患者。将 2 型糖尿病(糖尿病)患者与非糖尿病患者进行比较,应用多变量 Cox 回归模型和倾向评分匹配来评估 2 年时的主要预后终点——长期全因死亡率。次要预后终点包括 24 小时内的心脏性死亡、入院时的院内死亡、索引期的全因死亡率、索引期住院存活患者的 2 年时全因死亡率(即“出院后”)和 2 年时因复发性室性心动过速而再入院。
在 2411 例伴有 VT 的高危未匹配患者中,糖尿病的发生率为 25%(75%为非糖尿病患者)。两组患者的 VT(57% vs. 56%)和 VF(43% vs. 44%)发生率相似。多变量 Cox 回归模型显示,糖尿病与 2 年时的长期全因死亡率的主要终点相关(HR=1.513;p=0.001),这一结果在倾向评分匹配后仍然成立(46% vs. 33%,log-rank p=0.001;HR=1.525;p=0.001)。入院时伴有 VT 的患者中,院内死亡指数、30 天内全因死亡率以及出院后全因死亡率的次要终点发生率更高,但 24 小时内心脏性死亡和因复发性室性心动过速而再入院的发生率无差异。
入院时伴有 2 型糖尿病与伴有 VT 的患者的全因死亡率增加独立相关。