Department of Cardiovascular Medicine, Mayo Clinic, Rochester, MN, United States of America.
Department of Cardiovascular Medicine, Mayo Clinic, Rochester, MN, United States of America.
Int J Cardiol. 2019 Jan 1;274:232-236. doi: 10.1016/j.ijcard.2018.09.007. Epub 2018 Sep 5.
Dyspnea on exertion is common to both heart failure (HF) and chronic obstructive pulmonary disease (COPD), and it is important to discriminate whether symptoms are caused by HF or COPD in clinical practice. The ventilatory equivalent for carbon dioxide (V̇/V̇CO) slope and V̇ intercept (a reflection of pulmonary dead space) are two candidate non-invasive indices that could be used for this purpose. Thus, we compared non-invasive indexes of ventilatory efficiency in patients with HF and preserved or reduced ejection fraction (HFpEF and HFrEF, respectively) or COPD.
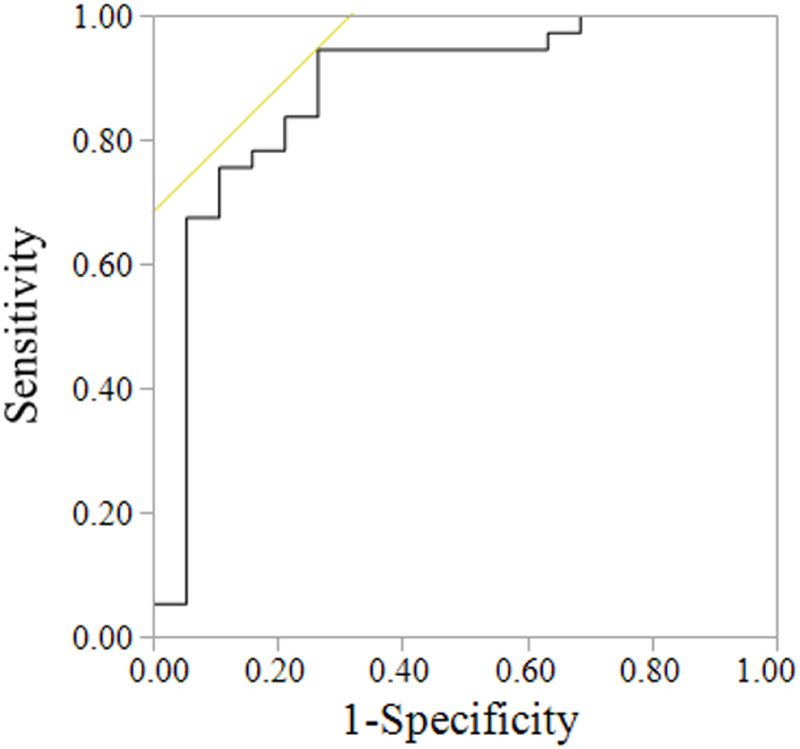
Patients with HFpEF (n = 21), HFrEF (n = 20), and COPD (n = 22) patients performed cardiopulmonary exercise testing to volitional fatigue. V̇ and gas exchange were measured via breath-by-breath open circuit spirometry. All data from rest to peak exercise were used to calculate V̇/V̇CO slope and V̇ intercept using linear regression. Receiver operating characteristic (ROC) curves were constructed to determine optimized cutoffs for V̇/V̇CO slope and V̇ intercept to discriminate HFpEF and HFrEF from COPD.
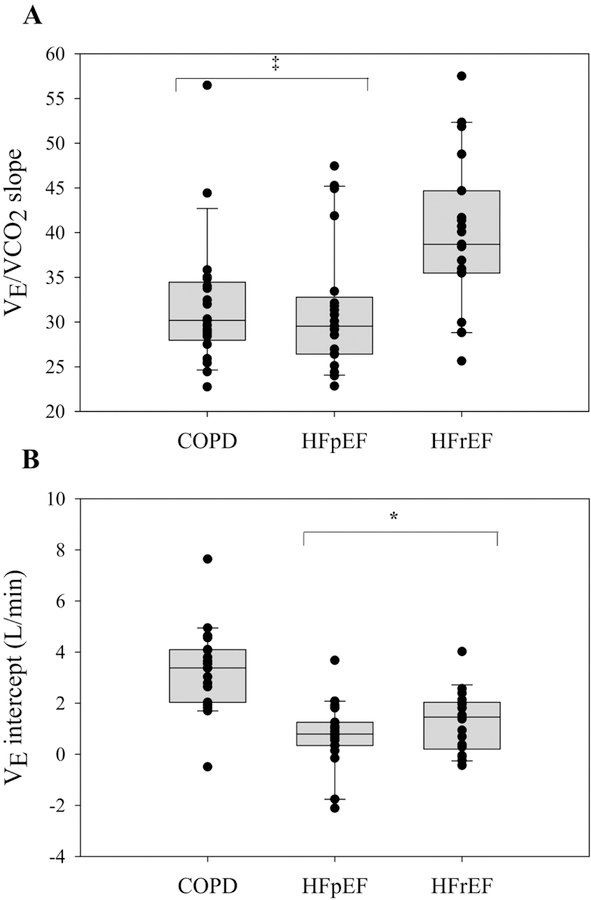
HFrEF patients had a greater V̇/V̇CO slope than HFpEF and COPD patients (HFrEF: 40 ± 9; HFpEF: 32 ± 7; COPD: 32 ± 7) (p < 0.01). COPD patients had a greater V̇ intercept than HFpEF and HFrEF patients (COPD: 3.32 ± 1.66; HFpEF: 0.77 ± 1.23; HFrEF: 1.28 ± 1.19 L/min) (p < 0.01). A V̇ intercept of 2.64 L/min discriminated COPD from HF patients (AUC: 0.88, p < 0.01), while V̇/V̇CO slope did not (p = 0.11).
These findings demonstrate that V̇ intercept, not V̇/V̇CO slope, may discriminate COPD from both HFpEF and HFrEF patients.
呼吸困难是心力衰竭(HF)和慢性阻塞性肺疾病(COPD)的共同症状,因此在临床实践中区分症状是由 HF 还是 COPD 引起非常重要。二氧化碳通气当量斜率(V̇/V̇CO)和 V̇截距(反映肺死腔)是两种可用于此目的的候选无创指标。因此,我们比较了 HF 患者(HFpEF 和 HFrEF,分别)和 COPD 患者的无创通气效率指标。
HFpEF 患者(n=21)、HFrEF 患者(n=20)和 COPD 患者(n=22)进行心肺运动试验直至疲劳。通过呼吸末闭路测功仪对 V̇和气体交换进行逐口气测量。使用线性回归从休息到运动峰值计算 V̇/V̇CO 斜率和 V̇截距。构建受试者工作特征(ROC)曲线,以确定 V̇/V̇CO 斜率和 V̇截距的最佳截断值,以区分 HFpEF 和 HFrEF 与 COPD。
HFrEF 患者的 V̇/V̇CO 斜率大于 HFpEF 和 COPD 患者(HFrEF:40±9;HFpEF:32±7;COPD:32±7)(p<0.01)。COPD 患者的 V̇截距大于 HFpEF 和 HFrEF 患者(COPD:3.32±1.66;HFpEF:0.77±1.23;HFrEF:1.28±1.19 L/min)(p<0.01)。V̇截距为 2.64 L/min 可区分 COPD 与 HF 患者(AUC:0.88,p<0.01),而 V̇/V̇CO 斜率则不能(p=0.11)。
这些发现表明,V̇截距而不是 V̇/V̇CO 斜率可能区分 COPD 与 HFpEF 和 HFrEF 患者。