Research Center Health Policy and Systems - International Health, School of Public Health, Université Libre de Bruxelles, Bruxelles, Belgium.
Department of Medicine and Therapeutics, University of Aberdeen, Aberdeen, Scotland, UK.
Nutr J. 2018 Sep 15;17(1):80. doi: 10.1186/s12937-018-0383-5.
The WHO recommended criteria for diagnosis of sever acute malnutrition (SAM) are weight-for-height/length Z-score (WHZ) of <- 3Z of the WHO standards, a mid-upper-arm circumference (MUAC) of < 115 mm, nutritional oedema or any combination of these parameters. A move to eliminate WHZ as a diagnostic criterion has been made on the assertion that children with a low WHZ are healthy, that MUAC is a "superior" prognostic indicator of mortality and that adding WHZ to the assessment does not improve the prediction of death. Our objective was to examine the literature comparing the risk of death of SAM children admitted by WHZ or MUAC criteria.
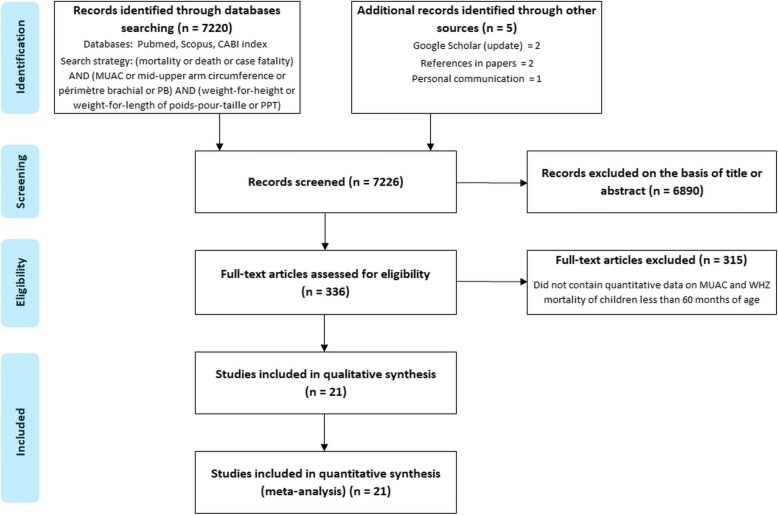
We conducted a systematic search for reports which examined the relationship of WHZ and MUAC to mortality for children less than 60 months. The WHZ, MUAC, outcome and programmatic variables were abstracted from the reports and examined. Individual study's case fatality rates were compared by chi-squared analysis and random effects meta-analyses for combined data.
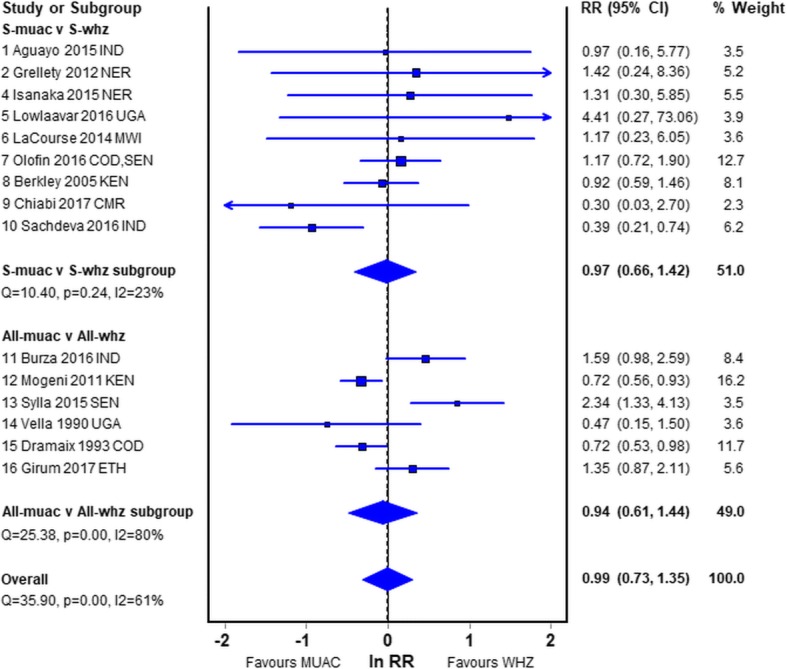
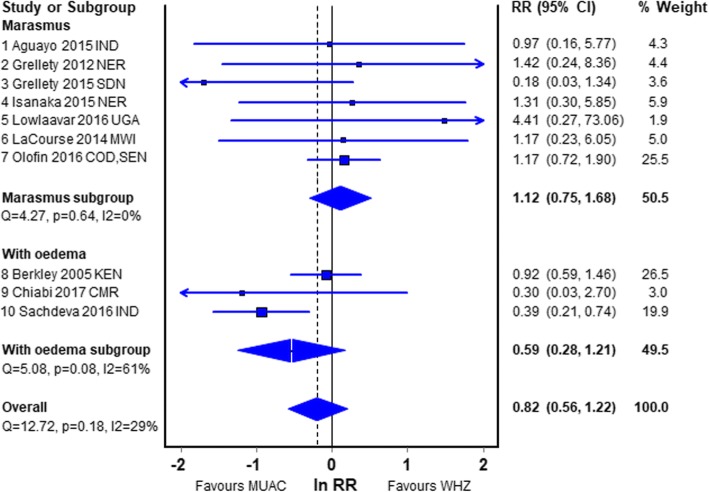
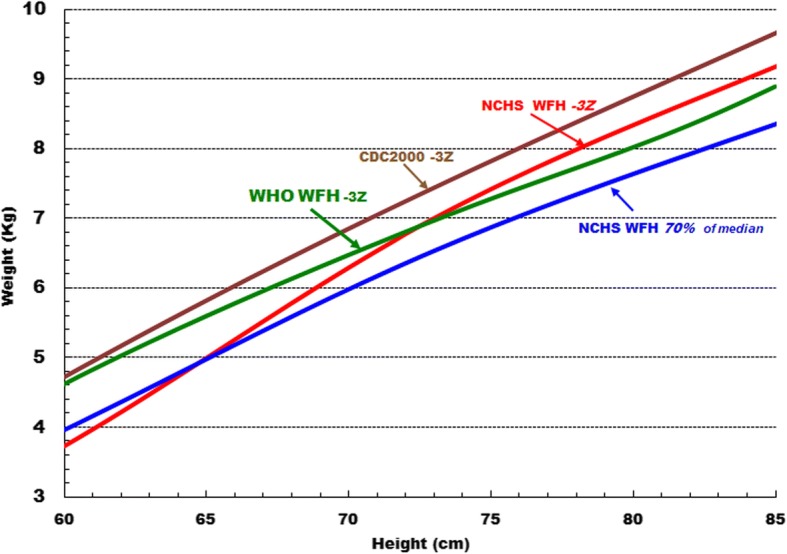
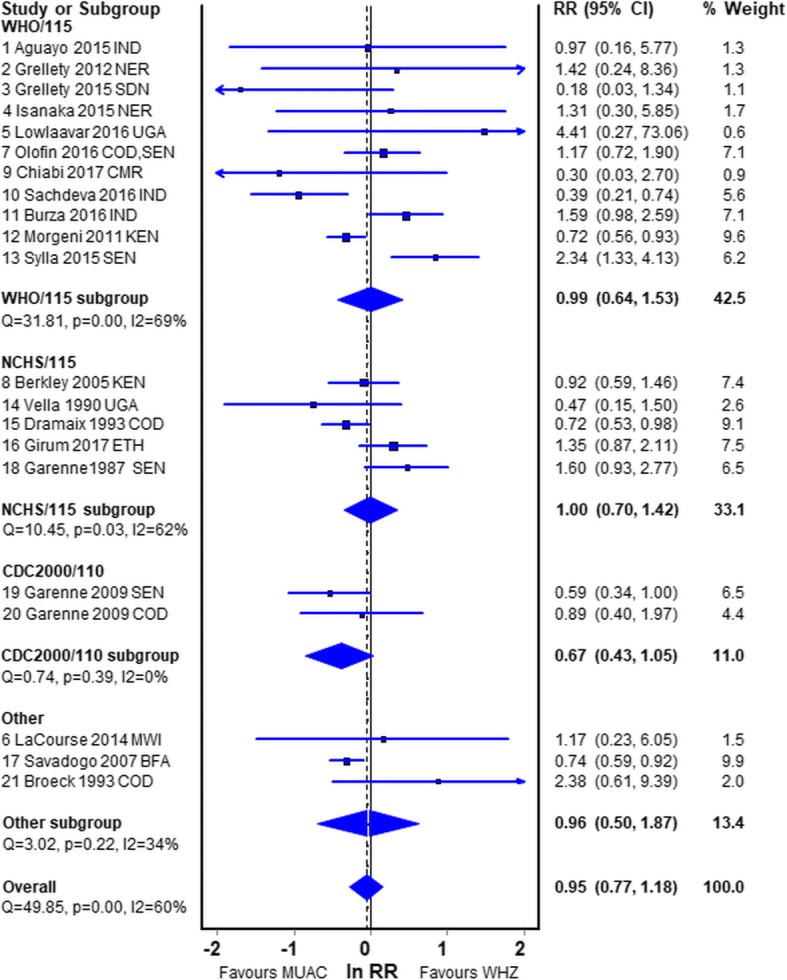
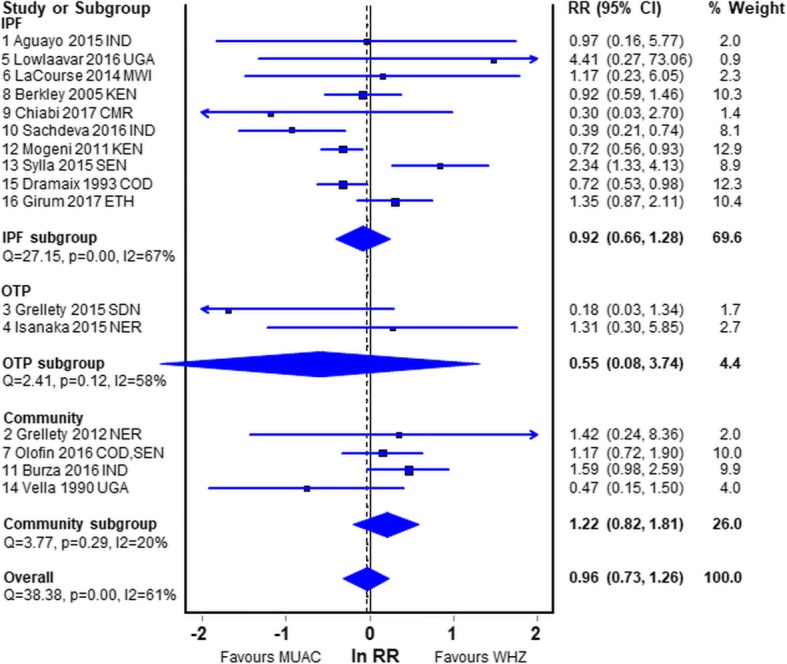
Twenty-one datasets were reviewed. All the patient studies had an ascertainment bias. Most were inadequate because they had insufficient deaths, used obsolete standards, combined oedematous and non-oedematous subjects, did not report the proportion of children with both deficits or the deaths occurred remotely after anthropometry. The meta-analyses showed that the mortality risks for children who have SAM by MUAC < 115 mm only and those with SAM by WHZ < -3Z only are not different.
As the diagnostic criteria identify different children, this analysis does not support the abandonment of WHZ as an important independent diagnostic criterion for the diagnosis of SAM. Failure to identify such children will result in their being denied treatment and unnecessary deaths from SAM.
世界卫生组织(WHO)推荐的严重急性营养不良(SAM)诊断标准为体重与身高/长度的 Z 评分(WHZ)<-3Z 低于 WHO 标准、中上臂围(MUAC)<115 毫米、营养性水肿或这些参数的任意组合。取消 WHZ 作为诊断标准的做法是基于以下断言:WHZ 低的儿童是健康的,MUAC 是死亡率的“优越”预后指标,并且在评估中添加 WHZ 并不能提高死亡预测的准确性。我们的目的是检查比较通过 WHZ 或 MUAC 标准入院的 SAM 儿童死亡风险的文献。
我们系统地搜索了检查 WHZ 和 MUAC 与 60 个月以下儿童死亡率之间关系的报告。从报告中提取 WHZ、MUAC、结局和方案变量并进行检查。通过卡方分析比较个别研究的病死率,并对合并数据进行随机效应荟萃分析。
共审查了 21 组数据集。所有患者研究都存在确定偏倚。大多数研究都是不充分的,因为它们的死亡人数不足,使用过时的标准,合并水肿和非水肿患者,未报告同时存在两种缺陷的儿童比例或死亡率是在人体测量后很久才发生的。荟萃分析表明,仅通过 MUAC <115 毫米诊断为 SAM 的儿童和仅通过 WHZ <-3Z 诊断为 SAM 的儿童的死亡率风险没有差异。
由于诊断标准识别出不同的儿童,因此该分析不支持放弃 WHZ 作为 SAM 诊断的重要独立诊断标准。未能识别出这些儿童将导致他们被拒绝治疗,并因 SAM 而不必要地死亡。