Cherutich Peter, Farquhar Carey, Wamuti Beatrice, Otieno Felix A, Ng'ang'a Ann, Mutiti Peter Maingi, Macharia Paul, Sambai Betsy, Bukusi David, Levin Carol
Ministry of Health, Afya House, Cathedral Road, P.O Box 30016-00100, Nairobi, Kenya.
Department of Global Health, University of Washington, Seattle, WA, USA.
BMC Health Serv Res. 2018 Sep 17;18(1):721. doi: 10.1186/s12913-018-3530-y.
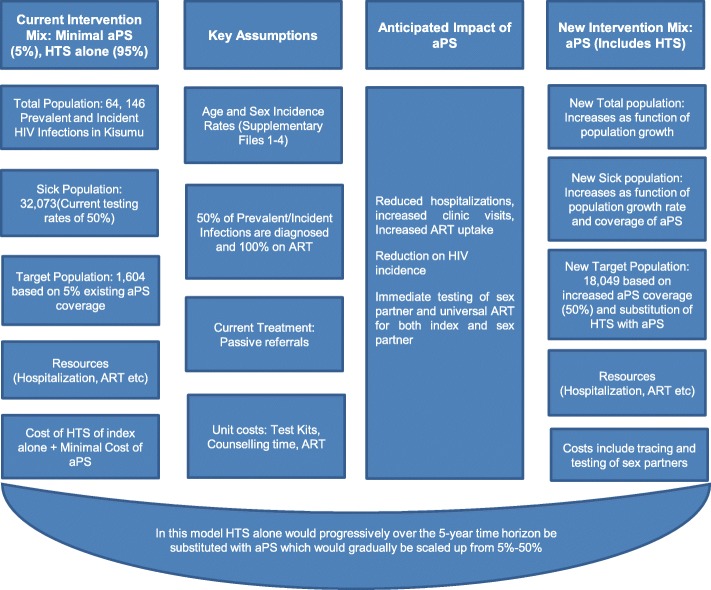
The elicitation of contact information, notification and testing of sex partners of HIV infected patients (aPS), is an effective HIV testing strategy in low-income settings but may not necessarily be affordable. We applied WHO guidelines and the International Society for Pharmaco-economics and Outcomes Research (ISPOR) guidelines to conduct cost and budget impact analyses, respectively, of aPS compared to current practice of HIV testing services (HTS) in Kisumu County, Kenya.
Using study data and time motion studies, we constructed an Excel-based tool to estimate costs and the budget impact of aPS. Cost data were collected from selected facilities in Kisumu County. We report the annual total and unit costs of HTS, incremental total and unit costs for aPS, and the budget impact of scaling up aPS over a 5-year horizon. We also considered a task-shifted scenario that used community health workers (CHWs) rather than facility based health workers and conducted sensitivity analyses assuming different rates of scale up of aPS.
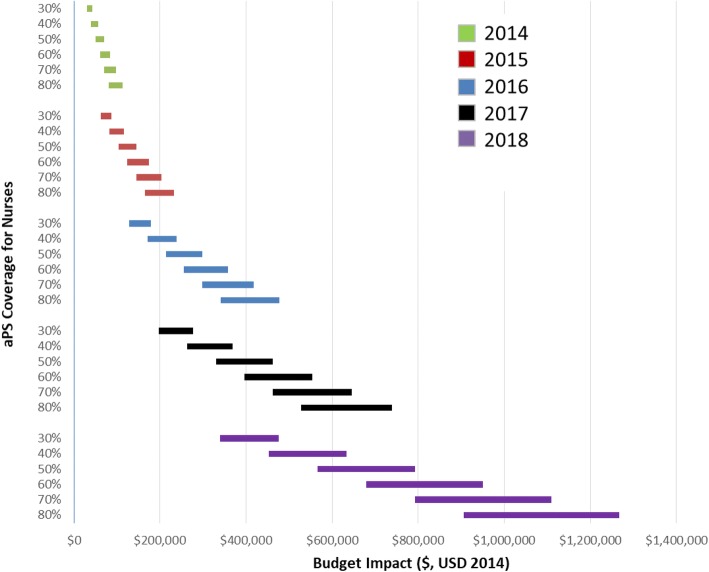
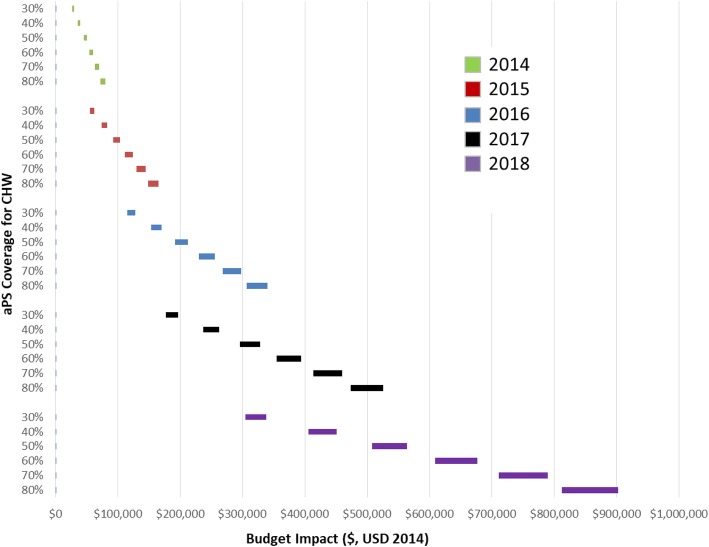
The average unit costs for HIV testing among HIV-infected index clients was US$ 25.36 per client and US$ 17.86 per client using nurses and CHWs, respectively. The average incremental costs for providing enhanced aPS in Kisumu County were US$ 1,092,161 and US$ 753,547 per year, using nurses and CHWs, respectively. The average incremental cost of scaling up aPS over a five period was 45% higher when using nurses compared to using CHWs (US$ 5,460,837 and US$ 3,767,738 respectively). Over the five years, the upper-bound budget impact of nurse-model was US$ 1,767,863, 63% and 35% of which were accounted for by aPS costs and ART costs, respectively. The CHW model incurred an upper-bound incremental cost of US$ 1,258,854, which was 71.2% lower than the nurse-based model. The budget impact was sensitive to the level of aPS coverage and ranged from US$ 28,547 for 30% coverage using CHWs in 2014 to US$ 1,267,603 for 80% coverage using nurses in 2018.
Scaling aPS using nurses has minimal budget impact but not cost-saving over a five-year period. Targeting aPS to newly-diagnosed index cases and task-shifting to community health workers is recommended.
获取艾滋病毒感染患者性伴侣的联系信息、进行通知及检测(aPS),在低收入环境中是一种有效的艾滋病毒检测策略,但不一定经济实惠。我们分别应用世界卫生组织指南和国际药物经济学与成果研究协会(ISPOR)指南,对肯尼亚基苏木县的aPS与当前艾滋病毒检测服务(HTS)的做法进行成本和预算影响分析。
利用研究数据和时间动作研究,我们构建了一个基于Excel的工具来估算aPS的成本和预算影响。成本数据从基苏木县选定的机构收集。我们报告了HTS的年度总成本和单位成本、aPS的增量总成本和单位成本,以及在5年期间扩大aPS规模的预算影响。我们还考虑了一种任务转移方案,即使用社区卫生工作者(CHW)而非机构内卫生工作者,并假设aPS不同的扩大规模率进行敏感性分析。
艾滋病毒感染的索引患者中,使用护士和CHW进行艾滋病毒检测的平均单位成本分别为每位患者25.36美元和17.86美元。在基苏木县提供强化aPS的平均增量成本,使用护士时分别为每年1,092,161美元,使用CHW时为每年753,547美元。与使用CHW相比,在五年期间扩大aPS规模时,使用护士的平均增量成本高出45%(分别为5,460,837美元和3,767,738美元)。在五年期间,护士模式的上限预算影响为1,767,863美元,其中aPS成本和抗逆转录病毒治疗成本分别占63%和35%。CHW模式产生的上限增量成本为1,258,854美元,比基于护士的模式低71.2%。预算影响对aPS的覆盖水平敏感,范围从2014年使用CHW覆盖率为30%时的28,547美元到2018年使用护士覆盖率为80%时的1,267,603美元。
使用护士扩大aPS规模在五年期间预算影响最小,但不节省成本。建议将aPS针对新诊断的索引病例,并将任务转移给社区卫生工作者。