Tsubosaka Masanori, Kaneyama Shuichi, Yano Tomonori, Kasahara Koichi, Kanemura Aritetsu, Takabatake Masato, Hirata Hiroaki, Sumi Masatoshi
Department of Orthopaedic Surgery, Kobe Rosai Hospital, 4-1-23, Kagoike-dori, Chuo-ku, Kobe, 651-0053, Japan.
Department of Orthopaedic Surgery, Hyogo Rehabilitation Centre Central Hospital, 1070 Akebono-cho, Nishi-ku, Kobe, 651-2181, Japan.
J Orthop Surg Res. 2018 Sep 18;13(1):239. doi: 10.1186/s13018-018-0947-2.
The treatment of lumbar spinal canal stenosis (LSS) depends on symptom severity. In the absence of severe symptoms such as severe motor disturbances or bowel and/or urinary dysfunction, conservative treatment is generally the first choice for the treatment of LSS. However, we experienced cases of worsening symptoms even after successful conservative treatment. The purpose of this study is to investigate the long-term clinical course of LSS following successful conservative treatment and analyze the prognostic factors associated with symptom deterioration.
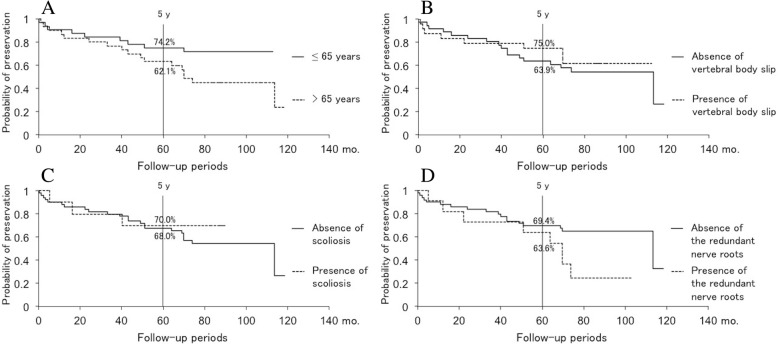
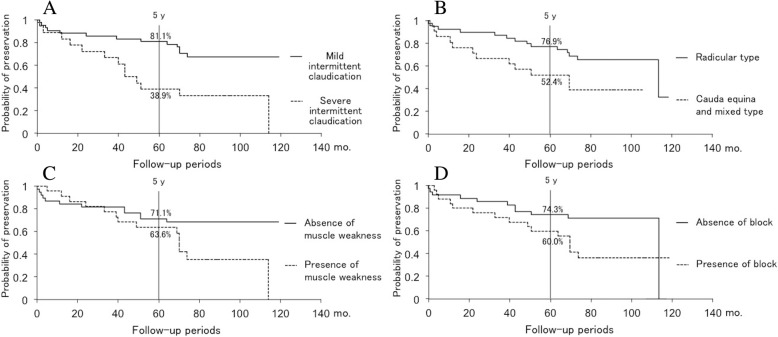
The study included 60 LSS patients (34 females and 26 males) whose symptoms were relieved by conservative treatment between April 2007 and March 2010 and who were followed up for 5 years or longer. The mean age at admission was 64.8 ± 8.5 years (range, 40-85 years old), and the mean follow-up period was 7.3 years (range, 5.8-9.5 years). We defined "deterioration" of symptoms as the shortening of intermittent claudication more than 50 m compared with those at discharge or the occurrence or progression of lower limb paralysis, and "poor outcome" as the deterioration within 5 years after discharge. The long-term outcome of conservative treatment for LSS was analyzed by Kaplan-Meier analysis. Furthermore, logistic regression analysis was performed to reveal the risk factors of poor outcome for clinical classification, severe intermittent claudication (≤ 100 m), lower limb muscle weakness, vertebral body slip (≥ 3 mm), scoliosis (Cobb angle ≥ 10°), block on myelography, and redundant nerve roots of the cauda equina.
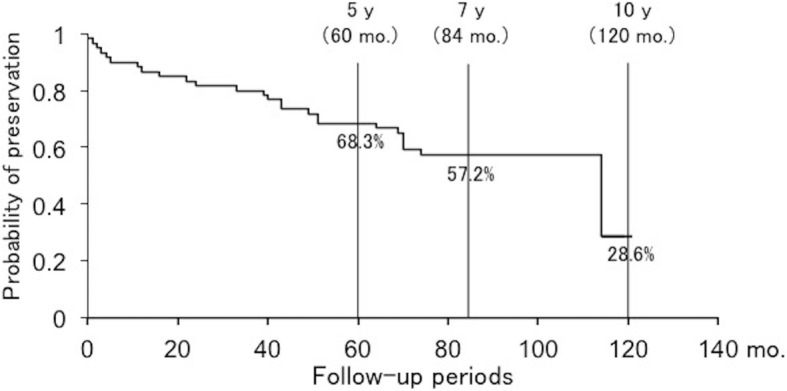
Thirty-four (56.7%) patients preserved their condition at discharge during the follow-up, whereas 26 patients (43.3%) showed deterioration. Sixteen patients had a decreased intermittent claudication distance, and 10 patients had newly developed or progressive paralysis. The probability of preservation was maintained at 68.3% at 5 years after discharge. Logistic regression analysis demonstrated that only severe intermittent claudication (≤ 100 m) was a significant risk factor of a poor outcome (p = 0.005, odds ratio = 6.665).
The patients with severe intermittent claudication should be carefully followed up because those are the significant deterioration candidates despite the success in conservative treatment.
腰椎管狭窄症(LSS)的治疗取决于症状严重程度。在没有严重症状如严重运动障碍或肠道和/或泌尿功能障碍的情况下,保守治疗通常是LSS治疗的首选。然而,我们遇到了即使在保守治疗成功后症状仍恶化的病例。本研究的目的是调查成功保守治疗后LSS的长期临床病程,并分析与症状恶化相关的预后因素。
本研究纳入了60例LSS患者(34例女性和26例男性),这些患者在2007年4月至2010年3月期间通过保守治疗症状得到缓解,并进行了5年或更长时间的随访。入院时的平均年龄为64.8±8.5岁(范围40 - 85岁),平均随访期为7.3年(范围5.8 - 9.5年)。我们将症状“恶化”定义为与出院时相比间歇性跛行距离缩短超过50米,或下肢瘫痪的发生或进展,将“预后不良”定义为出院后5年内症状恶化。通过Kaplan - Meier分析对LSS保守治疗的长期结果进行分析。此外,进行逻辑回归分析以揭示临床分类、严重间歇性跛行(≤100米)、下肢肌肉无力、椎体滑脱(≥3毫米)、脊柱侧凸(Cobb角≥10°)、脊髓造影阻滞和马尾神经根冗余等预后不良的危险因素。
34例(56.7%)患者在随访期间出院时病情保持稳定,而26例(43.3%)患者出现恶化。16例患者间歇性跛行距离缩短,10例患者出现新发或进行性瘫痪。出院后5年病情保持稳定的概率维持在68.3%。逻辑回归分析表明,只有严重间歇性跛行(≤100米)是预后不良的显著危险因素(p = 0.005,比值比 = 6.665)。
严重间歇性跛行的患者应仔细随访,因为尽管保守治疗成功,但这些患者是症状显著恶化的候选者。