Jiang Ye, Wang Li, Lao Jie, Zhao Xin
Department of Hand Surgery, Huashan Hospital, Fudan University; Key Laboratory of Hand Reconstruction, Ministry of Health; Shanghai Key Laboratory of Peripheral Nerve and Microsurgery, Shanghai, China.
Department of Hand Surgery, the Third Hospital of Hebei Medical University, Shijiazhuang, Hebei Province, China.
Neural Regen Res. 2018 Nov;13(11):1968-1973. doi: 10.4103/1673-5374.239444.
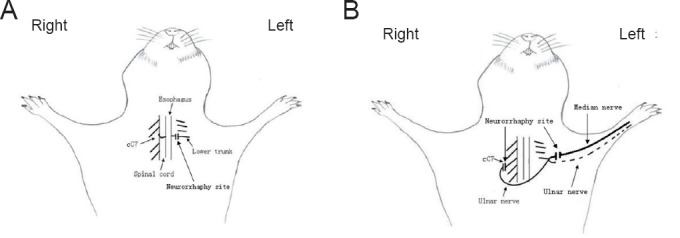
Contralateral C7 (cC7) root transfer to the healthy side is the main method for the treatment of brachial plexus root injury. A relatively new modification of this method involves cC7 root transfer to the lower trunk via the prespinal route. In the current study, we examined the effectiveness of this method using electrophysiological and histological analyses. To this end, we used a rat model of total brachial plexus injury, and cC7 root transfer was performed to either the lower trunk via the prespinal route or the median nerve via a subcutaneous tunnel to repair the injury. At 4, 8 and 12 weeks, the grasping test was used to measure the changes in grasp strength of the injured forepaw. Electrophysiological changes were examined in the flexor digitorum superficialis muscle. The change in the wet weight of the forearm flexor was also measured. Atrophy of the flexor digitorum superficialis muscle was assessed by hematoxylin-eosin staining. Toluidine blue staining was used to count the number of myelinated nerve fibers in the injured nerves. Compared with the traditional method, cC7 root transfer to the lower trunk via the prespinal route increased grasp strength of the injured forepaw, increased the compound muscle action potential maximum amplitude, shortened latency, substantially restored tetanic contraction of the forearm flexor muscles, increased the wet weight of the muscle, reduced atrophy of the flexor digitorum superficialis muscle, and increased the number of myelinated nerve fibers. These findings demonstrate that for finger flexion functional recovery in rats with total brachial plexus injury, transfer of the cC7 root to the lower trunk via the prespinal route is more effective than transfer to the median nerve via subcutaneous tunnel.
对侧C7(cC7)神经根转位至健侧是治疗臂丛神经根性损伤的主要方法。该方法一种相对较新的改良术式是经脊柱前入路将cC7神经根转位至下干。在本研究中,我们通过电生理和组织学分析来检验该方法的有效性。为此,我们使用了全臂丛神经损伤的大鼠模型,并经脊柱前入路将cC7神经根转位至下干或经皮下隧道转位至正中神经以修复损伤。在4周、8周和12周时,采用抓握试验测量受伤前爪抓握力的变化。检测指浅屈肌的电生理变化。还测量了前臂屈肌湿重的变化。通过苏木精-伊红染色评估指浅屈肌的萎缩情况。用甲苯胺蓝染色计数损伤神经中有髓神经纤维的数量。与传统方法相比,经脊柱前入路将cC7神经根转位至下干可增加受伤前爪的抓握力,增加复合肌肉动作电位的最大波幅,缩短潜伏期,显著恢复前臂屈肌的强直收缩,增加肌肉湿重,减轻指浅屈肌的萎缩,并增加有髓神经纤维的数量。这些结果表明,对于全臂丛神经损伤大鼠的手指屈曲功能恢复,经脊柱前入路将cC7神经根转位至下干比经皮下隧道转位至正中神经更有效。