Vanhaudenhuyse Audrey, Charland-Verville Vanessa, Thibaut Aurore, Chatelle Camille, Tshibanda Jean-Flory L, Maudoux Audrey, Faymonville Marie-Elisabeth, Laureys Steven, Gosseries Olivia
Department of Algology and Palliative Care, University Hospital of Liege, Liege, Belgium.
GIGA-Consciousness, Sensation & Perception Research Group, University of Liege, Liege, Belgium.
Front Neurol. 2018 Aug 28;9:671. doi: 10.3389/fneur.2018.00671. eCollection 2018.
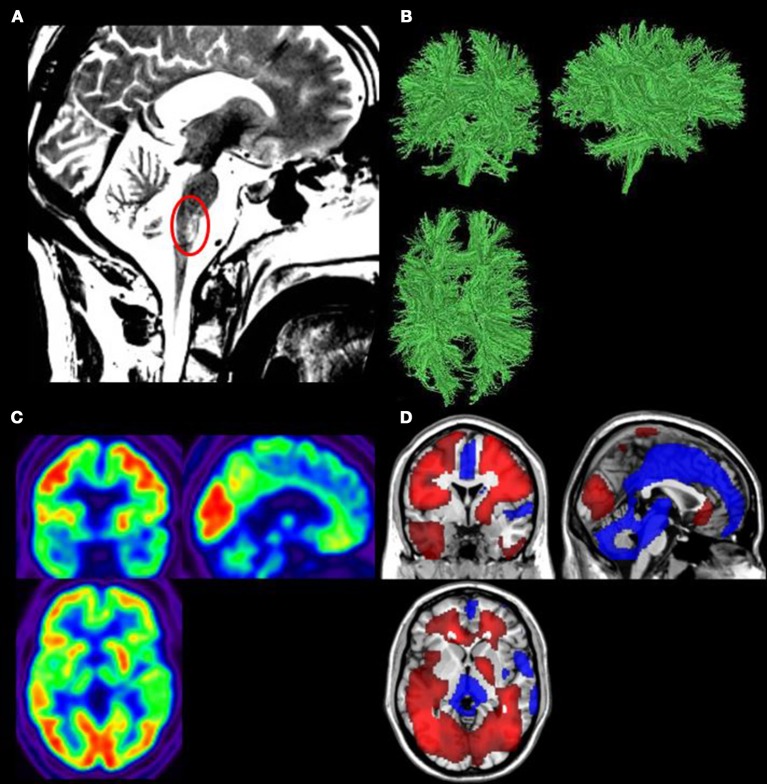
Despite recent advances in our understanding of consciousness disorders, accurate diagnosis of severely brain-damaged patients is still a major clinical challenge. We here present the case of a patient who was considered in an unresponsive wakefulness syndrome/vegetative state for 20 years. Repeated standardized behavioral examinations combined to neuroimaging assessments allowed us to show that this patient was in fact fully conscious and was able to functionally communicate. We thus revised the diagnosis into an incomplete locked-in syndrome, notably because the main brain lesion was located in the brainstem. Clinical examinations of severe brain injured patients suffering from serious motor impairment should systematically include repeated standardized behavioral assessments and, when possible, neuroimaging evaluations encompassing magnetic resonance imaging and F-fluorodeoxyglucose positron emission tomography.
尽管我们对意识障碍的理解最近取得了进展,但对严重脑损伤患者进行准确诊断仍然是一项重大的临床挑战。我们在此介绍一例被诊断为无反应觉醒综合征/植物状态长达20年的患者。反复进行的标准化行为检查与神经影像学评估相结合,使我们能够证明该患者实际上完全有意识,并且能够进行功能性交流。因此,我们将诊断修订为不完全闭锁综合征,特别是因为主要脑损伤位于脑干。对患有严重运动障碍的严重脑损伤患者进行临床检查时,应系统地包括反复进行的标准化行为评估,并在可能的情况下进行包括磁共振成像和F-氟脱氧葡萄糖正电子发射断层扫描在内的神经影像学评估。