Chestovich Paul J, McNicoll Christopher F, Fraser Douglas R, Patel Purvi P, Kuhls Deborah A, Clark Esmeralda, Fildes John J
Division of Acute Care Surgery, Department of Surgery, University of Nevada Las Vegas School of Medicine, Las Vegas, Nevada, USA.
Trauma Surg Acute Care Open. 2018 Aug 30;3(1):e000187. doi: 10.1136/tsaco-2018-000187. eCollection 2018.
Penetrating cardiac injuries (PCIs) are highly lethal, and a sternotomy is considered mandatory for suspected PCI. Recent literature suggests pericardial window (PCW) may be sufficient for superficial cardiac injuries to drain hemopericardium and assess for continued bleeding and instability. This study objective is to review patients with PCI managed with sternotomy and PCW and compare outcomes.
All patients with penetrating chest trauma from 2000 to 2016 requiring PCW or sternotomy were reviewed. Data were collected for patients who had PCW for hemopericardium managed with only pericardial drain, or underwent sternotomy for cardiac injuries grade 1-3 according to the American Association for the Surgery of Trauma (AAST) Cardiac Organ Injury Scale (OIS). The PCW+drain group was compared with the Sternotomy group using Fisher's exact and Wilcoxon rank-sum test with P<0.05 considered statistically significant.
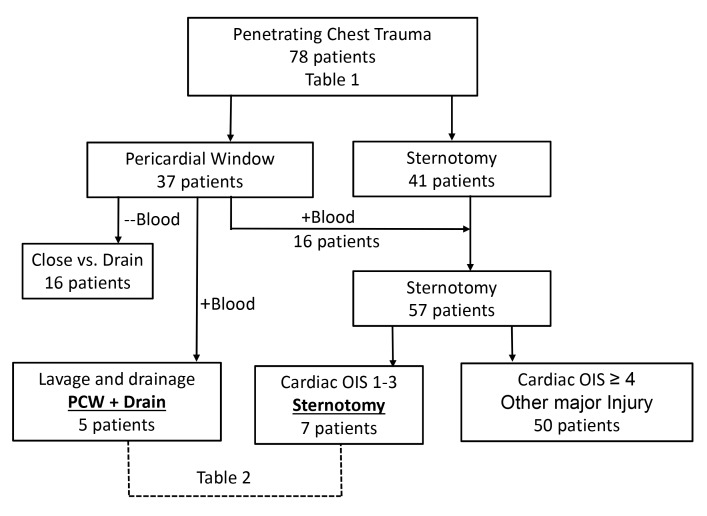
Sternotomy was performed in 57 patients for suspected PCI, including 7 with AAST OIS grade 1-3 injuries (Sternotomy group). Four patients had pericardial injuries, three had partial thickness cardiac injuries, two of which were suture-repaired. Average blood drained was 285 mL (100-500 mL). PCW was performed in 37 patients, and 21 had hemopericardium; 16 patients proceeded to sternotomy and 5 were treated with pericardial drainage (PCW+drain group). All PCW+drain patients had suction evacuation of hemopericardium, pericardial lavage, and verified bleeding cessation, followed by pericardial drain placement and admission to intensive care unit (ICU). Average blood drained was 240 mL (40-600 mL), and pericardial drains were removed on postoperative day 3.6 (2-5). There was no significant difference in demographics, injury mechanism, Revised Trauma Score exploratory laparotomies, hospital or ICU length of stay, or ventilator days. No in-hospital mortality occurred in either group.
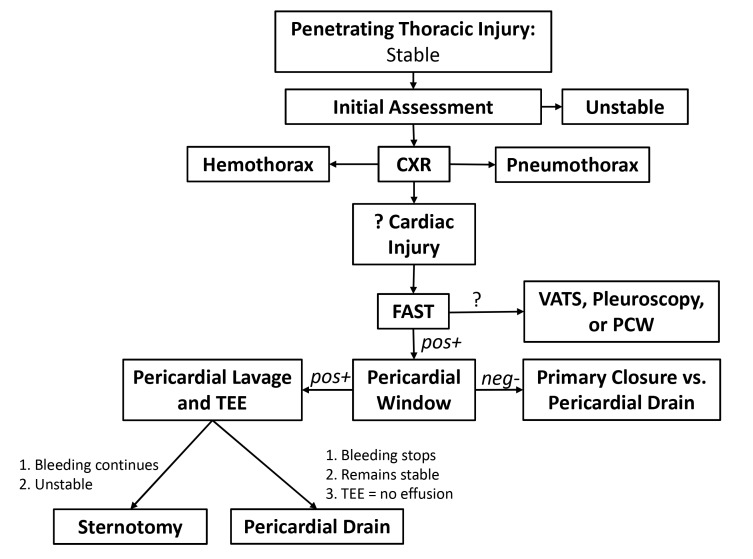
Hemodynamically stable patients with penetrating chest trauma and hemopericardium may be safely managed with PCW, lavage and drainage with documented cessation of bleeding, and postoperative ICU monitoring.
Therapeutic study, level IV.
穿透性心脏损伤(PCI)具有很高的致死率,对于疑似PCI患者,开胸手术被认为是必要的。近期文献表明,心包开窗术(PCW)可能足以处理浅表心脏损伤,以引流心包积血并评估是否持续出血及病情是否稳定。本研究的目的是回顾接受开胸手术和PCW治疗的PCI患者,并比较其治疗结果。
回顾了2000年至2016年所有因穿透性胸部创伤需要进行PCW或开胸手术的患者。收集了仅通过心包引流管治疗心包积血的PCW患者的数据,或根据美国创伤外科学会(AAST)心脏器官损伤量表(OIS)对1-3级心脏损伤患者进行开胸手术的数据。使用Fisher精确检验和Wilcoxon秩和检验将PCW+引流管组与开胸手术组进行比较,P<0.05被认为具有统计学意义。
57例疑似PCI患者接受了开胸手术,其中7例为AAST OIS 1-3级损伤(开胸手术组)。4例患者有心包损伤,3例有心脏部分厚度损伤,其中2例进行了缝合修复。平均引流量为285毫升(100-500毫升)。37例患者进行了PCW,21例有心包积血;16例患者随后进行了开胸手术,5例接受了心包引流(PCW+引流管组)。所有PCW+引流管组患者均进行了心包积血的负压引流、心包灌洗,并确认出血停止,随后放置心包引流管并入住重症监护病房(ICU)。平均引流量为240毫升(40-600毫升),心包引流管在术后第3.6天(2-5天)拔除。两组在人口统计学、损伤机制、修订创伤评分、剖腹探查术、住院或ICU住院时间或呼吸机使用天数方面无显著差异。两组均未发生院内死亡。
对于血流动力学稳定的穿透性胸部创伤伴心包积血患者,可通过PCW、灌洗和引流,并记录出血停止情况,以及术后ICU监测进行安全治疗。
治疗性研究,IV级。