Exercise Medicine Research Institute, Edith Cowan University, Joondalup, Western Australia, Australia.
School of Medical and Health Sciences, Edith Cowan University, Joondalup, Western Australia, Australia.
BJU Int. 2019 Feb;123(2):261-269. doi: 10.1111/bju.14505. Epub 2018 Sep 21.
To examine whether it is more efficacious to commence exercise medicine in men with prostate cancer at the onset of androgen-deprivation therapy (ADT) rather than later on during treatment to preserve bone and soft-tissue composition, as ADT results in adverse effects including: reduced bone mineral density (BMD), loss of muscle mass, and increased fat mass (FM).
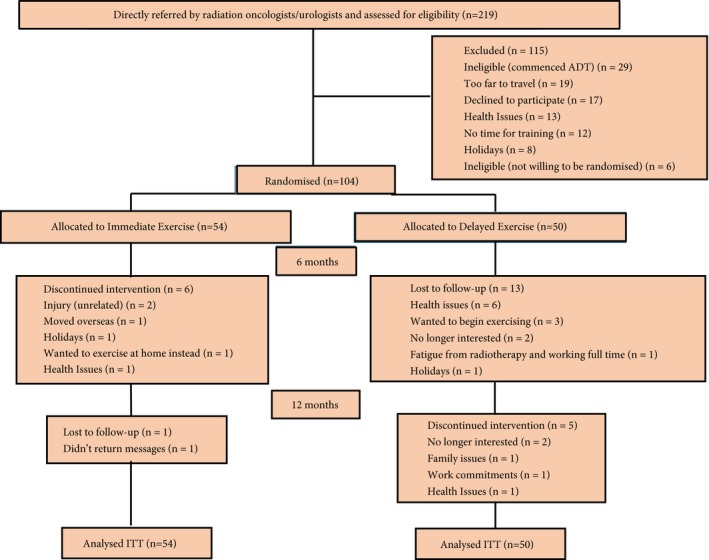
In all, 104 patients with prostate cancer, aged 48-84 years initiating ADT, were randomised to immediate exercise (IMEX, n = 54) or delayed exercise (DEL, n = 50) conditions. The former consisted of 6 months of supervised resistance/aerobic/impact exercise and the latter comprised 6 months of usual care followed by 6 months of the identical exercise programme. Regional and whole body BMD, lean mass (LM), whole body FM and trunk FM, and appendicular skeletal muscle (ASM) were assessed by dual X-ray absorptiometry, and muscle density by peripheral quantitative computed tomography at baseline, and at 6 and 12 months.
There was a significant time effect (P < 0.001) for whole body, spine and hip BMD with a progressive loss in the IMEX and DEL groups, although lumbar spine BMD was largely preserved in the IMEX group at 6 months compared with the DEL group (-0.4% vs -1.6%). LM, ASM, and muscle density were preserved in the IMEX group at 6 months, declined in the DEL group at 6 months (-1.4% to -2.5%) and then recovered at 12 months after training. FM and trunk FM increased (P < 0.001) over the 12-month period in the IMEX (7.8% and 4.5%, respectively) and DEL groups (6.5% and 4.3%, respectively).
Commencing exercise at the onset of ADT preserves lumbar spine BMD, muscle mass, and muscle density. To avoid treatment-related adverse musculoskeletal effects, exercise medicine should be prescribed and commenced at the onset of ADT.
研究在雄激素剥夺治疗(ADT)开始时开始运动医学治疗是否比在治疗过程中更能有效地保留男性前列腺癌患者的骨骼和软组织组成,因为 ADT 会导致包括以下在内的不良影响:骨密度(BMD)降低、肌肉量减少和脂肪量(FM)增加。
总共 104 名年龄在 48-84 岁之间开始 ADT 的前列腺癌患者被随机分配到即刻运动(IMEX,n=54)或延迟运动(DEL,n=50)条件。前者包括 6 个月的监督阻力/有氧/冲击运动,后者包括 6 个月的常规护理,然后是 6 个月的相同运动方案。通过双能 X 射线吸收法评估区域和全身 BMD、瘦体重(LM)、全身 FM 和躯干 FM 以及四肢骨骼肌(ASM),通过外周定量计算机断层扫描评估肌肉密度,基线、6 个月和 12 个月。
全身、脊柱和髋部 BMD 有显著的时间效应(P<0.001),IMEX 和 DEL 组均出现逐渐下降,但 IMEX 组在 6 个月时腰椎 BMD 与 DEL 组相比基本保持不变(-0.4%对-1.6%)。6 个月时,IMEX 组的 LM、ASM 和肌肉密度保持不变,DEL 组在 6 个月时下降(-1.4%至-2.5%),然后在训练后 12 个月恢复。在 IMEX(分别为 7.8%和 4.5%)和 DEL 组(分别为 6.5%和 4.3%)中,12 个月期间 FM 和躯干 FM 增加(P<0.001)。
在 ADT 开始时进行运动可保留腰椎 BMD、肌肉量和肌肉密度。为了避免与治疗相关的不良肌肉骨骼影响,应在 ADT 开始时开具并开始运动医学治疗。