Department of Anesthesiology, Critical Care and Pain Medicine, Boston Children's Hospital and Harvard Medical School, Boston, MA.
Department of Neurology, Boston Children's Hospital and Harvard Medical School, Boston, MA.
Crit Care Med. 2018 Dec;46(12):e1160-e1166. doi: 10.1097/CCM.0000000000003434.
Time-averaged intracranial pressure-to-blood pressure Fisher-transformed Pearson correlation (PRx) is used to assess cerebral autoregulation and derive optimal cerebral perfusion pressure. Empirically, impaired cerebral autoregulation is considered present when PRx is positive; greater difference between time series median cerebral perfusion pressure and optimal cerebral perfusion pressure (ΔCPP) is associated with worse outcomes. Our aims are to better understand: 1) the potential strategies for targeting optimal cerebral perfusion pressure; 2) the relationship between cerebral autoregulation and PRx; and 3) the determinants of greater ΔCPP.
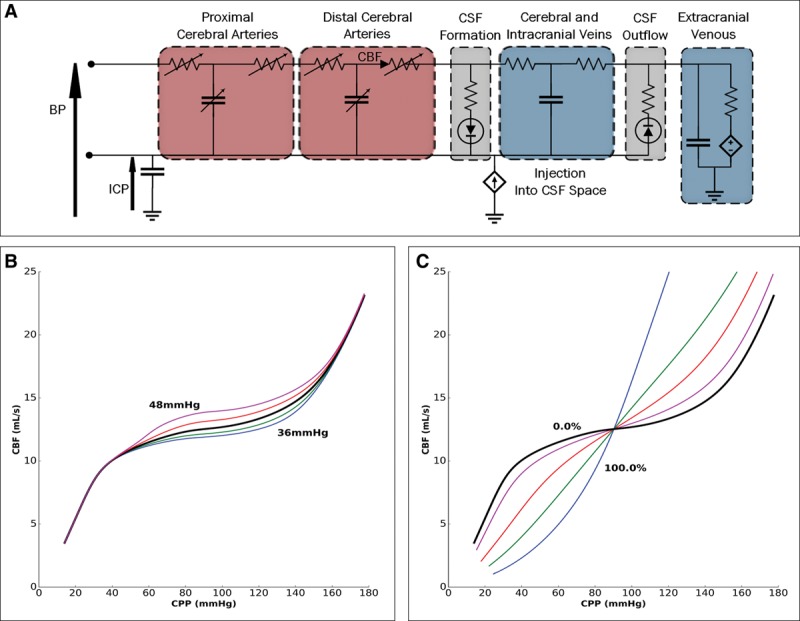
Mechanistic simulation using a lumped compartmental model of blood pressure, intracranial pressure, cerebral autoregulation, cerebral blood volume, PaCO2, and cerebral blood flow.
University critical care integrative modeling and precision physiology research group.
None, in silico studies.
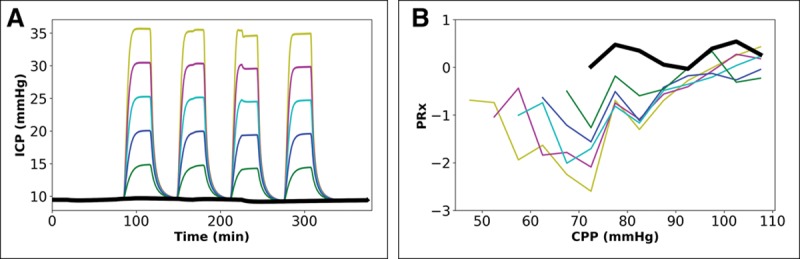
Simulations in blood pressure, intracranial pressure, PaCO2, and impairment of cerebral autoregulation, with examination of "output" cerebral perfusion pressure versus PRx-plots, optimal cerebral perfusion pressure, and ΔCPP.
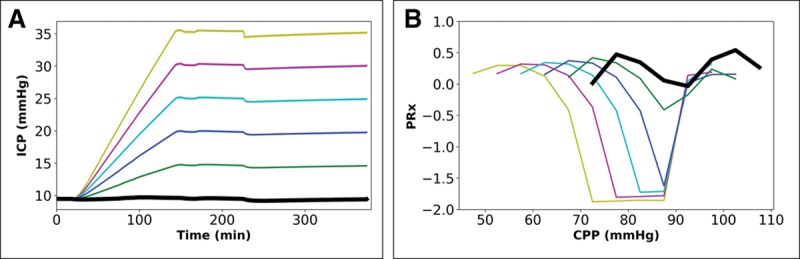
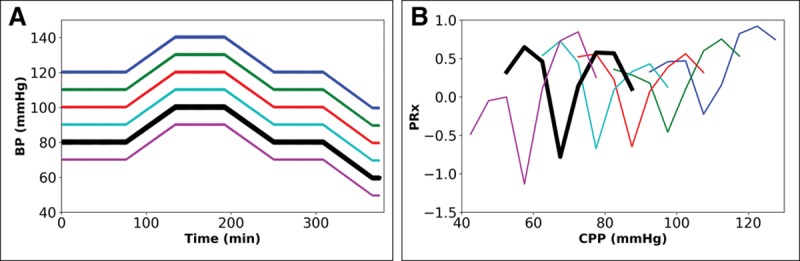
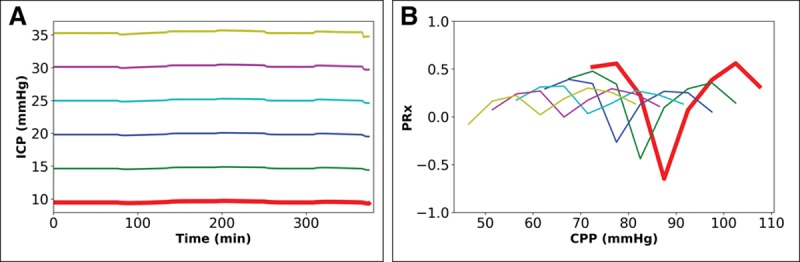
In regard to targeting optimal cerebral perfusion pressure, a shift in mean blood pressure or mean intracranial pressure with no change in mean blood pressure, with intact cerebral autoregulation, impacts optimal cerebral perfusion pressure. Second, a positive PRx occurs even with intact cerebral autoregulation. In relation to ΔCPP, for a given input blood pressure profile, with constant intracranial pressure, altering the degree of impairment in cerebral autoregulation or the level of PaCO2 maintains differences to within ±5 mm Hg. Change in intracranial pressure due to either an intermittently prolonged pattern of raised intracranial pressure or terminal escalation shows ΔCPP greater than 10 mm Hg and less than -10 mm Hg, respectively.
These mechanistic simulations provide insight into the empiric basis of optimal cerebral perfusion pressure and the significance of PRx and ΔCPP. PRx and optimal cerebral perfusion pressure deviations do not directly reflect changes in cerebral autoregulation but are, in general, related to the presence of complex states involving well-described clinical progressions with raised intracranial pressure.
时间平均颅内压与血压 Fisher 变换 Pearson 相关系数(PRx)用于评估脑自动调节并得出最佳脑灌注压。经验上,当 PRx 为正时,认为脑自动调节受损;时间序列中脑灌注压中位数与最佳脑灌注压(ΔCPP)之间的差异越大,预后越差。我们的目的是更好地理解:1)靶向最佳脑灌注压的潜在策略;2)脑自动调节与 PRx 的关系;3)更大 ΔCPP 的决定因素。
使用血压、颅内压、脑自动调节、脑血容量、PaCO2 和脑血流的集中式容积模型进行机制模拟。
大学重症监护综合建模和精准生理学研究组。
无,体内研究。
模拟血压、颅内压、PaCO2 和脑自动调节受损,并检查“输出”脑灌注压与 PRx 图、最佳脑灌注压和 ΔCPP 的关系。
关于靶向最佳脑灌注压,平均血压或平均颅内压的变化而平均血压不变,脑自动调节完整,会影响最佳脑灌注压。其次,即使脑自动调节完整,也会出现正 PRx。关于 ΔCPP,对于给定的输入血压曲线,颅内压恒定,改变脑自动调节受损程度或 PaCO2 水平可使差异保持在±5mmHg 以内。由于颅内压间歇性延长或终末期升高引起的颅内压变化分别导致 ΔCPP 大于 10mmHg 和小于-10mmHg。
这些机制模拟为最佳脑灌注压的经验基础以及 PRx 和 ΔCPP 的意义提供了深入了解。PRx 和最佳脑灌注压偏差并不直接反映脑自动调节的变化,但通常与涉及具有升高颅内压的明确临床进展的复杂状态有关。