Department of Nephrology, Ajou University School of Medicine, Suwon, Korea.
Department of Emergency Medicine, Ajou University School of Medicine, Suwon, Korea.
PLoS One. 2018 Oct 4;13(10):e0204586. doi: 10.1371/journal.pone.0204586. eCollection 2018.
We aimed to develop a model of chronic kidney disease (CKD) progression for predicting the probability and time to progression from various CKD stages to renal replacement therapy (RRT), using 6 months of clinical data variables routinely measured at healthcare centers.
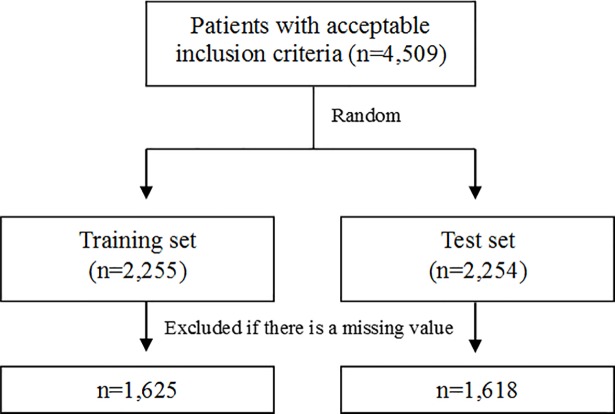
Data were derived from the electronic medical records of Ajou University Hospital, Suwon, South Korea from October 1997 to September 2012. We included patients who were diagnosed with CKD (estimated glomerular filtration rate [eGFR] < 60 mL·min-1·1.73 m-2 for ≥ 3 months) and followed up for at least 6 months. The study population was randomly divided into training and test sets.
We identified 4,509 patients who met reasonable diagnostic criteria. Patients were randomly divided into 2 groups, and after excluding patients with missing data, the training and test sets included 1,625 and 1,618 patients, respectively. The integral mean was the most powerful explanatory (R2 = 0.404) variable among the 8 modified values. Ten variables (age, sex, diabetes mellitus[DM], polycystic kidney disease[PKD], serum albumin, serum hemoglobin, serum phosphorus, serum potassium, eGFR (calculated by Chronic Kidney Disease Epidemiology Collaboration [CKD-EPI]), and urinary protein) were included in the final risk prediction model for CKD stage 3 (R2 = 0.330). Ten variables (age, sex, DM, GN, PKD, serum hemoglobin, serum blood urea nitrogen[BUN], serum calcium, eGFR(calculated by Modification of Diet in Renal Disease[MDRD]), and urinary protein) were included in the final risk prediction model for CKD stage 4 (R2 = 0.386). Four variables (serum hemoglobin, serum BUN, eGFR(calculated by MDRD) and urinary protein) were included in the final risk prediction model for CKD stage 5 (R2 = 0.321).
We created a prediction model according to CKD stages by using integral means. Based on the results of the Brier score (BS) and Harrel's C statistics, we consider that our model has significant explanatory power to predict the probability and interval time to the initiation of RRT.
我们旨在开发一种慢性肾脏病(CKD)进展模型,以预测从各种 CKD 阶段进展到肾脏替代治疗(RRT)的概率和时间,使用在医疗保健中心常规测量的 6 个月临床数据变量。
数据来自韩国水原市 Ajou 大学医院的电子病历,时间为 1997 年 10 月至 2012 年 9 月。我们纳入了被诊断为 CKD(估计肾小球滤过率[eGFR]<60 mL·min-1·1.73 m-2 持续≥3 个月)并至少随访 6 个月的患者。研究人群被随机分为训练集和测试集。
我们确定了符合合理诊断标准的 4509 名患者。患者被随机分为 2 组,在排除缺失数据的患者后,训练集和测试集分别包含 1625 名和 1618 名患者。积分均值是 8 个修正值中最具解释力(R2 = 0.404)的变量。10 个变量(年龄、性别、糖尿病[DM]、多囊肾病[PKD]、血清白蛋白、血清血红蛋白、血清磷、血清钾、eGFR(由慢性肾脏病流行病学合作研究[CKD-EPI]计算)和尿蛋白)被纳入 CKD 3 期风险预测模型(R2 = 0.330)。10 个变量(年龄、性别、DM、GN、PKD、血清血红蛋白、血清尿素氮[BUN]、血清钙、eGFR(由肾脏病饮食改良研究[MDRD]计算)和尿蛋白)被纳入 CKD 4 期风险预测模型(R2 = 0.386)。4 个变量(血清血红蛋白、血清 BUN、eGFR(由 MDRD 计算)和尿蛋白)被纳入 CKD 5 期风险预测模型(R2 = 0.321)。
我们根据 CKD 阶段使用积分均值创建了一个预测模型。基于 Brier 评分(BS)和 Harrel's C 统计结果,我们认为我们的模型对预测开始 RRT 的概率和时间间隔具有显著的解释能力。