Nuffield Department of Primary Care Health Sciences, University of Oxford, Radcliffe Primary Care Building, Radcliffe Observatory Quarter, Woodstock Road, Oxford, 0X2 6GG, UK.
Division of General Internal Medicine, Johns Hopkins University School of Medicine, Baltimore, 21205, USA.
J Cancer Surviv. 2018 Dec;12(6):803-812. doi: 10.1007/s11764-018-0717-5. Epub 2018 Oct 6.
Overlooking other medical conditions during cancer treatment and follow-up could result in excess morbidity and mortality, thereby undermining gains associated with early detection and improved treatment of cancer. We compared the quality of care for diabetes patients subsequently diagnosed with breast, colorectal, or prostate cancer to matched, diabetic non-cancer controls.
Longitudinal cohort study using primary care records from the Clinical Practice Research Datalink, United Kingdom. Patients with pre-existing diabetes were followed for up to 5 years after cancer diagnosis, or after an assigned index date (non-cancer controls). Quality of diabetes care was estimated based on Quality and Outcomes Framework indicators. Mixed effects logistic regression analyses were used to compare the unadjusted and adjusted odds of meeting quality measures between cancer patients and controls, overall and stratified by type of cancer.
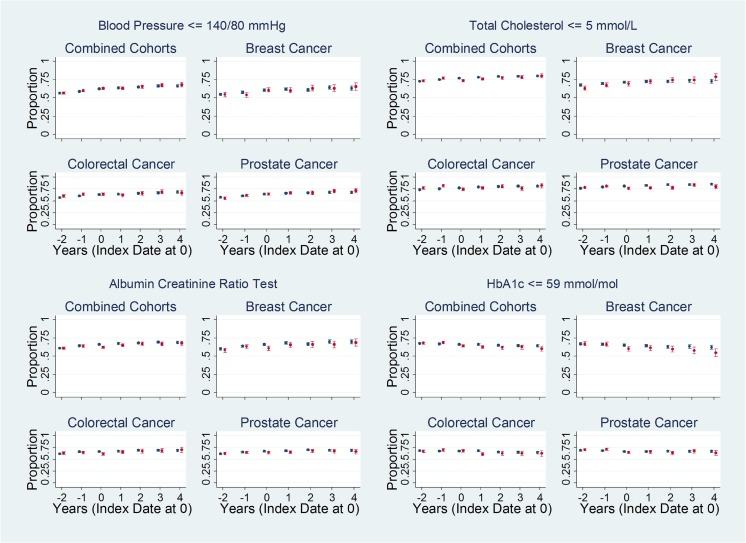
3382 cancer patients and 11,135 controls contributed 44,507 person-years of follow-up. In adjusted analyses, cancer patients were less likely to meet five of 14 quality measures, including: total cholesterol ≤ 5 mmol/L (odds ratio [OR] = 0.82; 95% confidence interval [CI], 0.75-0.90); glycosylated hemoglobin ≤ 59 mmol/mol (adjusted OR = 0.77; 95% CI, 0.70-0.85); and albumin creatinine ratio testing (adjusted OR = 0.83; 95% CI, 0.75-0.91). However, cancer patients were as likely as their matched controls to meet quality measures for other diabetes services, including retinal screening, foot examination, and dietary review.
Although in the short-term, cancer patients were less likely to achieve target thresholds for cholesterol and HbA1c, they continued to receive high-quality diabetes primary care throughout 5 years post diagnosis.
These findings are important for cancer survivors with pre-existing diabetes because they indicate that high-quality diabetes care is maintained throughout the continuum of cancer diagnosis, treatment, and follow-up.
在癌症治疗和随访期间忽视其他医疗状况可能导致发病率和死亡率过高,从而破坏早期发现和改善癌症治疗带来的益处。我们比较了随后被诊断患有乳腺癌、结直肠癌或前列腺癌的糖尿病患者与匹配的、无癌症的糖尿病对照患者的护理质量。
这是一项使用英国临床实践研究数据链接中的初级保健记录进行的纵向队列研究。患有糖尿病的患者在癌症诊断后最长 5 年内或在指定的索引日期(非癌症对照)后接受随访。根据质量和结果框架指标评估糖尿病护理质量。使用混合效应逻辑回归分析比较癌症患者和对照组之间总体以及按癌症类型分层的不符合质量措施的未调整和调整比值比。
3382 名癌症患者和 11135 名对照者共提供了 44507 人年的随访。在调整后的分析中,癌症患者有五个而非 14 个质量指标的达标可能性较小,包括:总胆固醇≤5mmol/L(比值比[OR]=0.82;95%置信区间[CI],0.75-0.90);糖化血红蛋白≤59mmol/mol(调整后 OR=0.77;95% CI,0.70-0.85);白蛋白肌酐比值检测(调整后 OR=0.83;95% CI,0.75-0.91)。然而,癌症患者与他们匹配的对照者一样有可能达到其他糖尿病服务的质量标准,包括视网膜筛查、足部检查和饮食评估。
尽管在短期内,癌症患者达到胆固醇和糖化血红蛋白目标阈值的可能性较小,但在诊断后 5 年内,他们继续接受高质量的糖尿病初级保健。
这些发现对患有糖尿病的癌症幸存者很重要,因为它们表明在癌症诊断、治疗和随访的整个过程中,高质量的糖尿病护理得以维持。