Ifakara Health Institute, P.O. Box 78373, Dar es Salaam, Tanzania.
Boyd Orr Centre for Population and Ecosystem Health, Institute of Biodiversity, Animal Health and Comparative Medicine, University of Glasgow, UK.
Vaccine. 2019 Oct 3;37 Suppl 1(Suppl 1):A45-A53. doi: 10.1016/j.vaccine.2018.08.086. Epub 2018 Oct 8.
Rabies is preventable through prompt administration of post-exposure prophylaxis (PEP) to exposed persons, but PEP access is limited in many rabies-endemic countries. We investigated how access to PEP can be improved to better prevent human rabies.
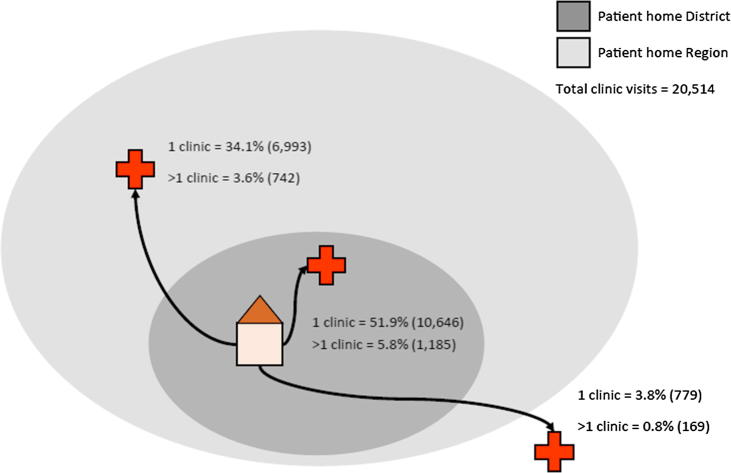
Using data from different settings in Tanzania, including contact tracing (2,367 probable rabies exposures identified) and large-scale mobile phone-based surveillance (24,999 patient records), we estimated the incidence of rabies exposures and bite-injuries, and examined health seeking and health outcomes in relation to PEP access. We used surveys and qualitative interviews with stakeholders within the health system to further characterise PEP supply and triangulate these findings.
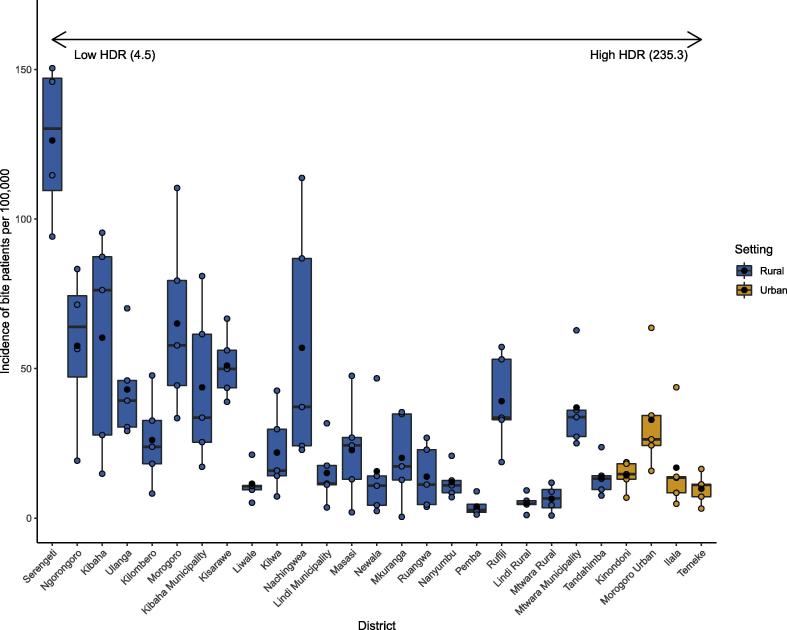
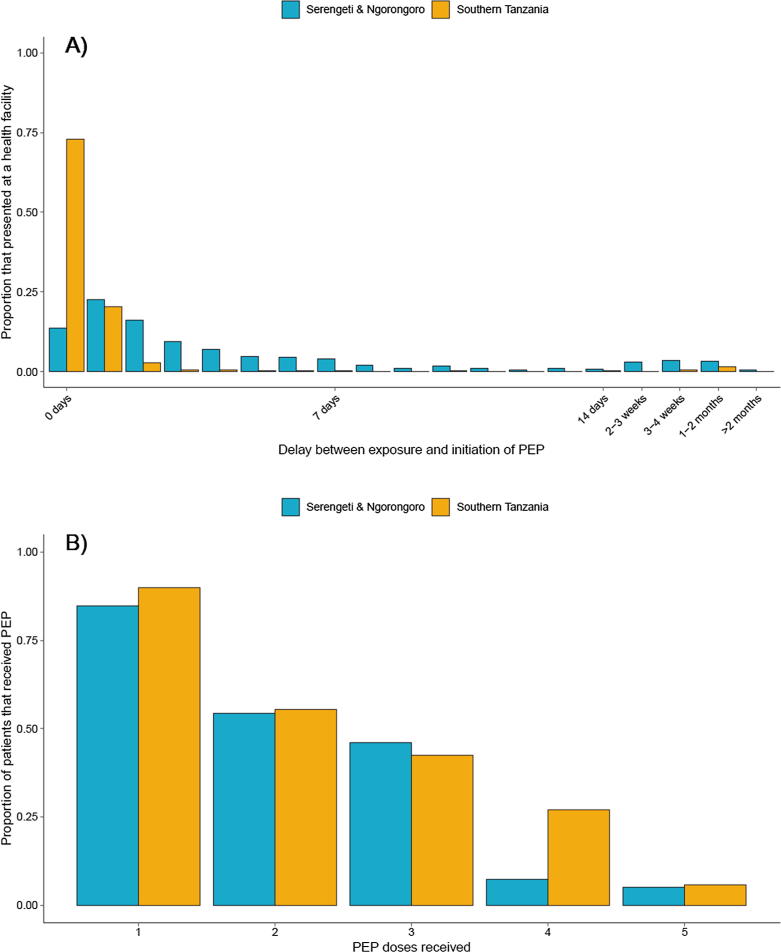
Incidence of bite-injury patients was related to dog population sizes, with higher incidence in districts with lower human:dog ratios and urban centres. A substantial percentage (25%) of probable rabies exposures did not seek care due to costs and limited appreciation of risk. Upon seeking care a further 15% of probable rabies exposed persons did not obtain PEP due to shortages, cost barriers or misadvice. Of those that initiated PEP, 46% did not complete the course. If no PEP was administered, the risk of developing rabies following a probable rabies exposure was high (0.165), with bites to the head carrying most risk. Decentralized and free PEP increased the probability that patients received PEP and reduced delays in initiating PEP. No major difficulties were encountered by health workers whilst switching to dose-sparing ID administration of PEP. Health infrastructure also includes sufficient cold chain capacity to support improved PEP provision. However, high costs to governments and patients currently limits the supply chain and PEP access. The cost barrier was exacerbated by decentralization of budgets, with priority given to purchase of cheaper medicines for other conditions. Reactive procurement resulted in limited and unresponsive PEP supply, increasing costs and risks to bite victims.
PEP access could be improved and rabies deaths reduced through ring-fenced procurement, switching to dose-sparing ID regimens and free provision of PEP.
狂犬病可通过及时对暴露者进行暴露后预防(PEP)来预防,但在许多狂犬病流行国家,PEP 的可及性有限。我们研究了如何改善 PEP 的可及性,以更好地预防人类狂犬病。
利用来自坦桑尼亚不同环境的数据,包括接触者追踪(确定了 2367 例可能的狂犬病暴露)和基于移动电话的大规模监测(24999 例患者记录),我们估计了狂犬病暴露和咬伤的发生率,并检查了与 PEP 可及性相关的卫生服务寻求和卫生结果。我们使用调查和与卫生系统内利益攸关方的定性访谈,进一步描述 PEP 供应,并对这些发现进行三角验证。
咬伤患者的发病率与犬只数量有关,在人类与犬只比例较低的地区和城市中心发病率较高。由于费用和对风险认识有限,相当大比例(25%)的可能狂犬病暴露者没有寻求治疗。在寻求治疗后,由于短缺、费用障碍或错误建议,进一步有 15%的可能狂犬病暴露者没有获得 PEP。在开始接受 PEP 的人中,有 46%没有完成疗程。如果未给予 PEP,在可能的狂犬病暴露后发生狂犬病的风险很高(0.165),头部咬伤风险最大。分散和免费的 PEP 增加了患者获得 PEP 的可能性,并减少了开始 PEP 的延迟。在改用剂量节约型 ID 管理 PEP 时,卫生工作者没有遇到任何重大困难。卫生基础设施还包括足够的冷链能力,以支持改善 PEP 的供应。然而,政府和患者的高成本目前限制了供应链和 PEP 的可及性。预算的分散化使成本障碍更加严重,因为优先考虑购买更便宜的其他疾病药物。反应性采购导致 PEP 供应有限且无响应,增加了咬伤受害者的成本和风险。
通过专用采购、改用剂量节约型 ID 方案和免费提供 PEP,可以改善 PEP 的可及性并减少狂犬病死亡。