Institute of Biodiversity, Animal Health & Comparative Medicine, University of Glasgow, Glasgow G12 8QQ, UK.
Department of the Control of Neglected Tropical Diseases, 1121 Geneva 27, Switzerland.
Vaccine. 2019 Oct 3;37 Suppl 1(Suppl 1):A166-A173. doi: 10.1016/j.vaccine.2018.11.010. Epub 2018 Dec 7.
The Strategic Advisory Group of Experts (SAGE) Working Group on rabies vaccines and immunoglobulins was established in 2016 to develop practical and feasible recommendations for prevention of human rabies. To support the SAGE agenda we developed models to compare the relative costs and potential benefits of rabies prevention strategies.
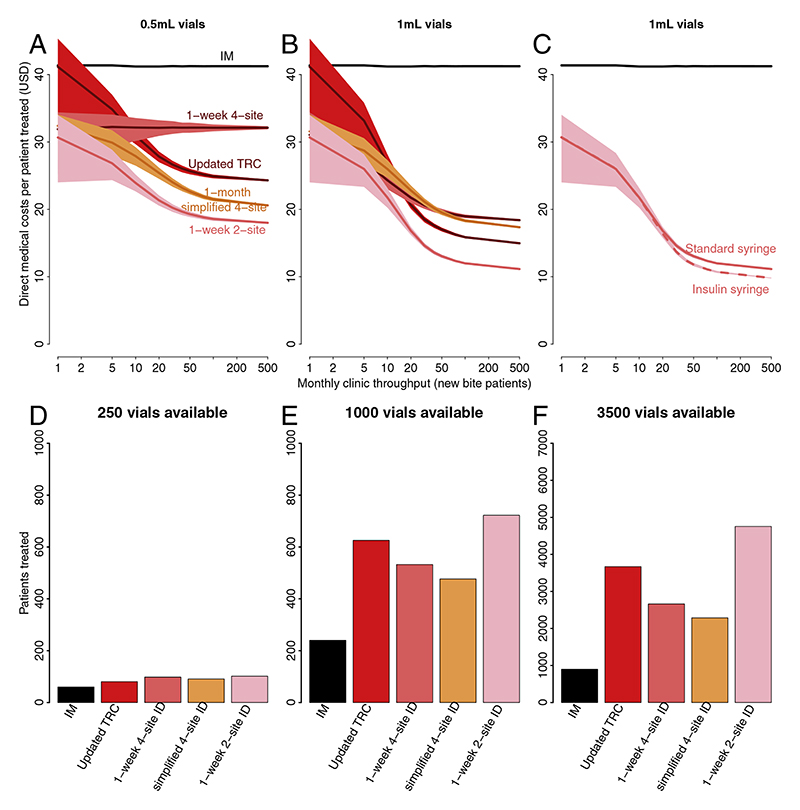
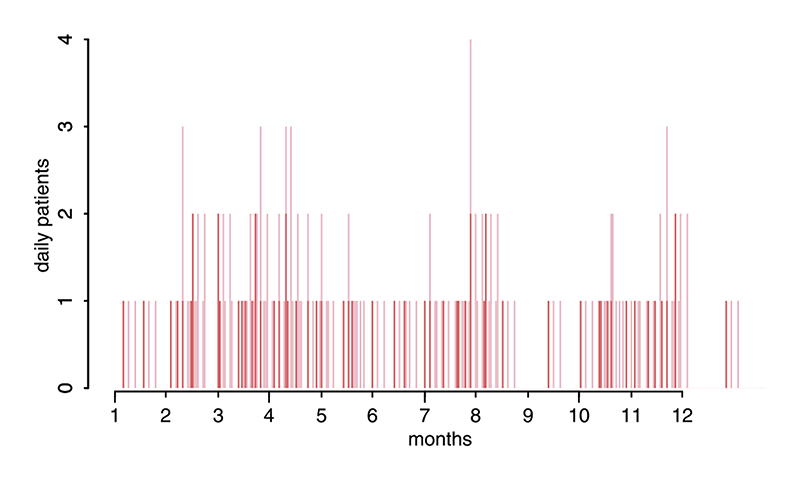
We examined Post-Exposure Prophylaxis (PEP) regimens, protocols for administration of Rabies Immunoglobulin (RIG) and inclusion of rabies Pre-Exposure Prophylaxis (PrEP) within the Expanded Programme on Immunization (EPI). For different PEP regimens, clinic throughputs and consumables for vaccine administration, we evaluated the cost per patient treated, costs to patients and potential to treat more patients given limited vaccine availability.
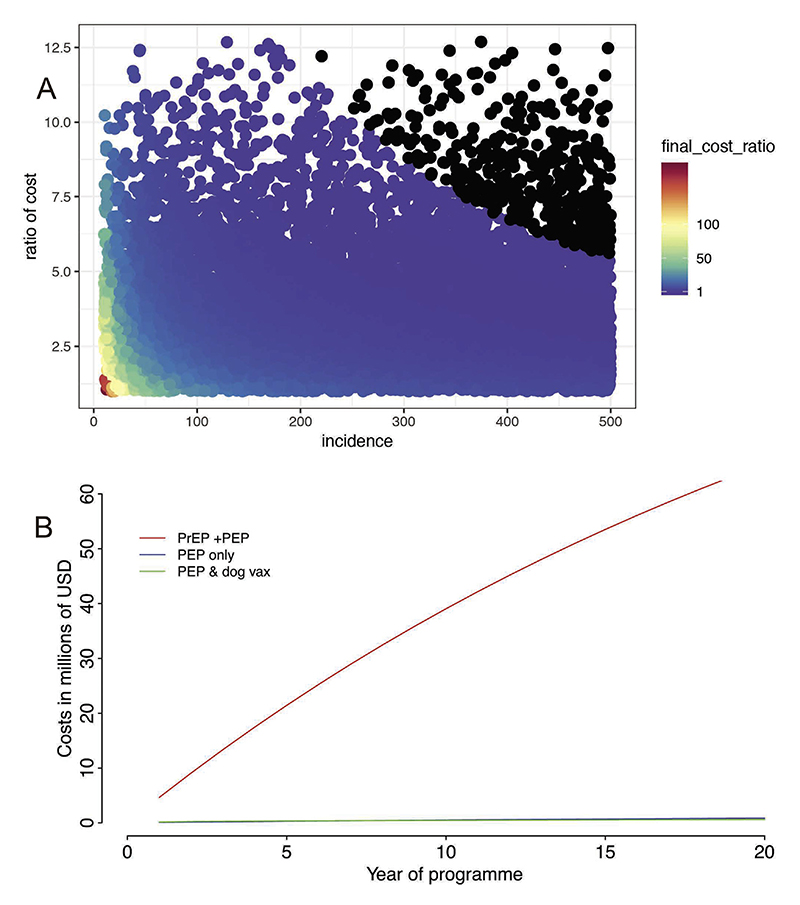
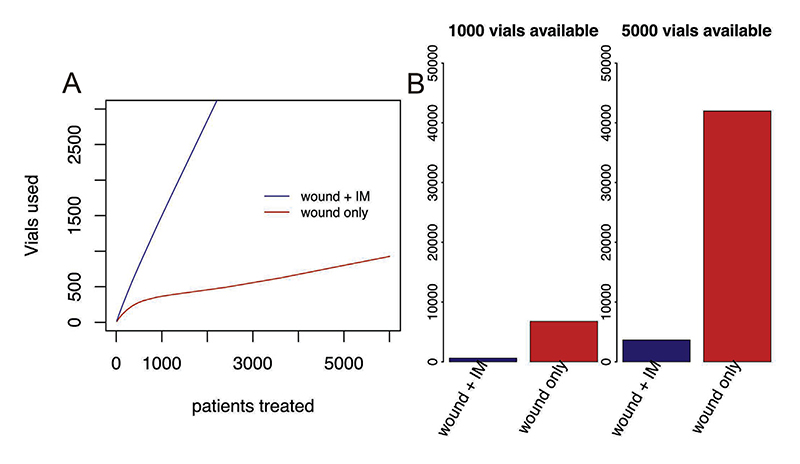
We found that intradermal (ID) vaccination reduces the volume of vaccine used in all settings, is less costly and has potential to mitigate vaccine shortages. Specifically, the abridged 1-week 2-site ID regimen was the most cost-effective PEP regimen, even in settings with low numbers of bite patients presenting to clinics. We found advantages of administering RIG to the wound(s) only, using considerably less product than when the remaining dose is injected intramuscularly distant to the wound(s). We found that PrEP as part of the EPI programme would be substantially more expensive than use of PEP and dog vaccination in prevention of human rabies.
These modeling insights inform WHO recommendations for use of human rabies vaccines and biologicals. Specifically, the 1-week 2-site ID regimen is recommended as it is less costly and treats many more patients when vaccine is in short supply. If available, RIG should be administered at the wound only. PrEP is highly unlikely to be an efficient use of resources and should therefore only be considered in extreme circumstances, where the incidence of rabies exposures is extremely high.
战略咨询专家组(SAGE)狂犬病疫苗和免疫球蛋白工作组于 2016 年成立,旨在为预防人类狂犬病制定实用可行的建议。为支持 SAGE 议程,我们开发了模型来比较狂犬病预防策略的相对成本和潜在收益。
我们检查了暴露后预防(PEP)方案、狂犬病免疫球蛋白(RIG)的管理方案以及将狂犬病暴露前预防(PrEP)纳入扩大免疫规划(EPI)。对于不同的 PEP 方案、疫苗接种的诊所吞吐量和消耗品,我们评估了每位治疗患者的成本、患者的成本以及在疫苗供应有限的情况下治疗更多患者的潜力。
我们发现皮内(ID)接种在所有情况下都减少了疫苗的使用量,成本更低,并有潜力缓解疫苗短缺。具体来说,缩短的 1 周 2 部位 ID 方案是最具成本效益的 PEP 方案,即使在向诊所就诊的咬伤患者数量较少的情况下也是如此。我们发现,仅将 RIG 施用于伤口(s)具有优势,使用的产品比将剩余剂量注射到伤口(s)远处的肌肉内时要少得多。我们发现,PrEP 作为 EPI 计划的一部分,在预防人类狂犬病方面的成本将大大高于使用 PEP 和犬类疫苗。
这些建模结果为世卫组织关于使用人类狂犬病疫苗和生物制品的建议提供了信息。具体来说,建议使用 1 周 2 部位 ID 方案,因为在疫苗供应短缺时,它的成本更低,治疗的患者更多。如果有,RIG 应仅在伤口处施用。PrEP 极不可能成为资源的有效利用,因此仅应在狂犬病暴露发生率极高的极端情况下考虑。