Centre for Rehabilitation Research, Nuffield Department of Rhuematology, Orthopaedics and Musculskeletal Sciences, University of Oxford, Oxford, UK.
Oxford Clinical Trials Research Unit, Centre for Statistics in Medicine, Nuffield Department of Orthopaedics, Rheumatology and Musculoskeletal Sciences, University of Oxford, Oxford, UK.
BMJ Open. 2018 Oct 18;8(10):e022205. doi: 10.1136/bmjopen-2018-022205.
Neurogenic claudication due to spinal stenosis is common in older adults. The effectiveness of conservative interventions is not known. The aim of the study is to estimate the clinical and cost-effectiveness of a physiotherapist-delivered, combined physical and psychological intervention.
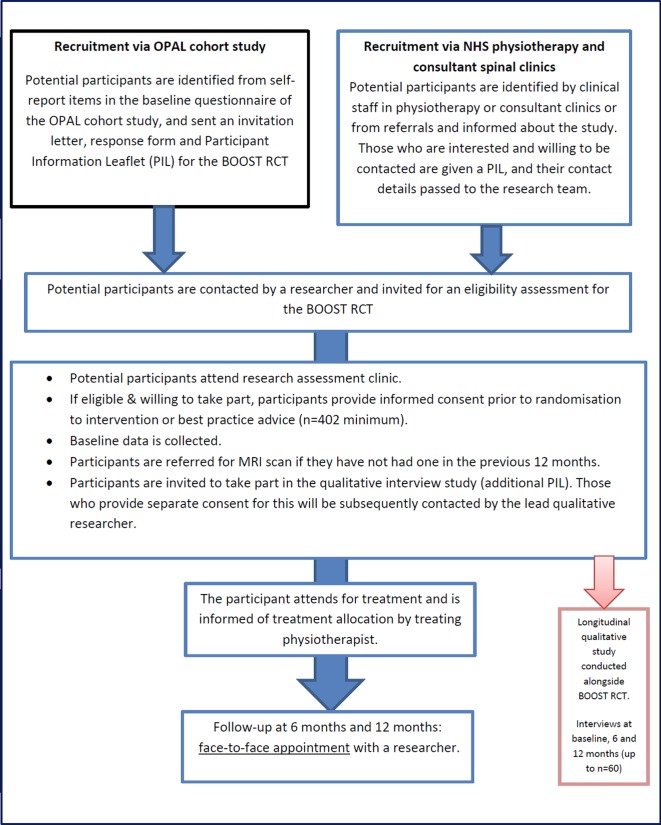
This is a pragmatic, multicentred, randomised controlled trial. Participants are randomised to a combined physical and psychological intervention (Better Outcomes for Older people with Spinal Trouble (BOOST) programme) or best practice advice (control). Community-dwelling adults, 65 years and over, with neurogenic claudication are identified from community and secondary care services. Recruitment is supplemented using a primary care-based cohort. Participants are registered prospectively and randomised in a 2:1 ratio (intervention:control) using a web-based service to ensure allocation concealment. The target sample size is a minimum of 402. The BOOST programme consists of an individual assessment and twelve 90 min classes, including education and discussion underpinned by cognitive behavioural techniques, exercises and walking circuit. During and after the classes, participants undertake home exercises and there are two support telephone calls to promote adherence with the exercises. Best practice advice is delivered in one to three individual sessions with a physiotherapist. The primary outcome is the Oswestry Disability Index at 12 months. Secondary outcomes include the 6 Minute Walk Test, Short Physical Performance Battery, Fear Avoidance Beliefs Questionnaire and Gait Self-Efficacy Scale. Outcomes are measured at 6 and 12 months by researchers who are masked to treatment allocation. The primary statistical analysis will be by 'intention to treat'. There is a parallel health economic evaluation and qualitative study.
Ethical approval was given on 3 March 2016 (National Research Ethics Committee number: 16/LO/0349). This protocol adheres to the Standard Protocol Items: Recommendations for Interventional Trials checklist. The results will be reported at conferences and in peer-reviewed publications using the Consolidated Standards of Reporting Trials guidelines. A plain English summary will be published on the BOOST website.
ISRCTN12698674; Pre-results.
由椎管狭窄引起的神经性跛行在老年人中很常见。目前尚不清楚保守干预的效果。本研究旨在评估由物理治疗师提供的结合生理和心理干预措施的临床和成本效益。
这是一项实用的、多中心的、随机对照试验。参与者被随机分配到联合物理和心理干预(BOOST 计划)或最佳实践建议(对照组)。从社区和二级保健服务中确定患有神经性跛行的 65 岁及以上的社区居住成年人。使用基于初级保健的队列补充招募。参与者使用基于网络的服务进行前瞻性登记和 2:1 随机分组(干预组:对照组),以确保分配隐藏。目标样本量最小为 402 例。BOOST 计划包括个人评估和十二节 90 分钟的课程,包括教育和讨论,以认知行为技术为基础,辅以锻炼和步行循环。在课程期间和之后,参与者进行家庭锻炼,并进行两次支持电话以促进对锻炼的依从性。最佳实践建议在与物理治疗师的一到三次个别会议中提供。主要结果是 12 个月时的 Oswestry 残疾指数。次要结果包括 6 分钟步行测试、简短身体表现电池、恐惧回避信念问卷和步态自我效能量表。由对治疗分配不知情的研究人员在 6 个月和 12 个月时进行测量。主要统计分析将按“意向治疗”进行。还有并行的健康经济学评估和定性研究。
2016 年 3 月 3 日获得了国家伦理委员会的批准(编号:16/LO/0349)。本方案符合干预试验标准建议清单。结果将在会议上和同行评审出版物中报告,使用 CONSORT 报告指南。根据简化报告标准的建议,将在 BOOST 网站上发布一份通俗易懂的摘要。
ISRCTN8674;预结果。