Shen Colette J, Kummerlowe Megan N, Redmond Kristin J, Martinez-Gutierrez Juan Carlos, Usama Syed Muhammad, Holdhoff Matthias, Grossman Stuart A, Laterra John J, Strowd Roy E, Kleinberg Lawrence R
Department of Radiation Oncology, Johns Hopkins University School of Medicine, Baltimore, Maryland.
Department of Radiation Oncology, University of North Carolina School of Medicine, Chapel Hill, North Carolina.
Adv Radiat Oncol. 2018 Jul 10;3(4):582-590. doi: 10.1016/j.adro.2018.06.005. eCollection 2018 Oct-Dec.
Reirradiation for recurrent glioma remains controversial without knowledge of optimal patient selection, dose, fractionation, and normal tissue tolerances. We retrospectively evaluated outcomes and toxicity after conventionally fractionated reirradiation for recurrent high-grade glioma, along with the impact of concurrent chemotherapy.
We conducted a retrospective review of patients reirradiated for high-grade glioma recurrence between 2007 and 2016 (including patients with initial low-grade glioma). Outcome metrics included overall survival (OS), prognostic factors for survival, and treatment-related toxicity.
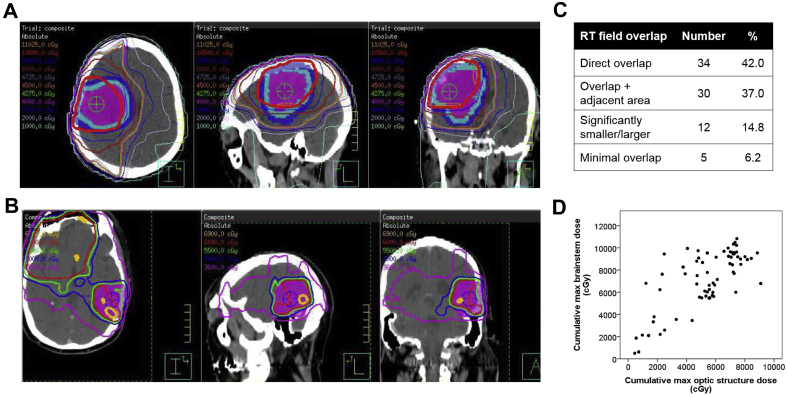
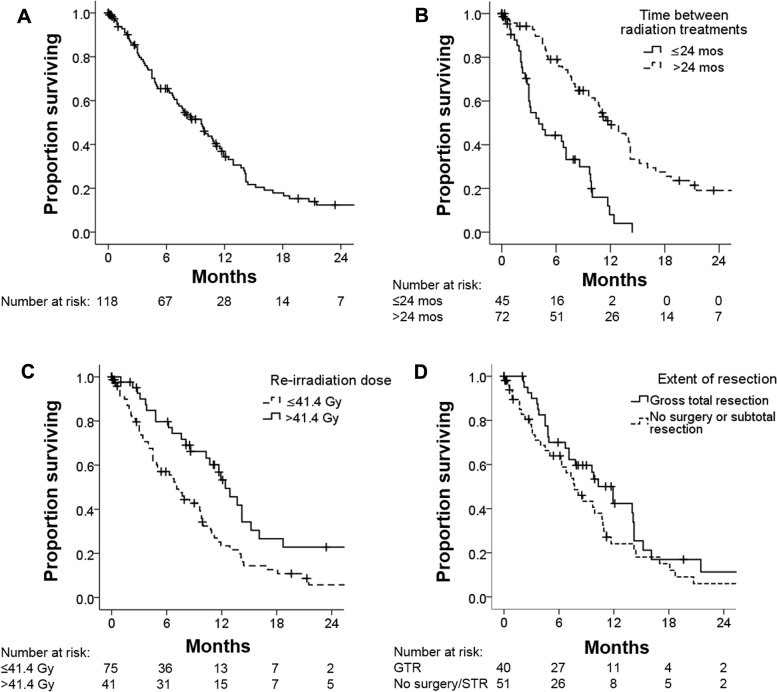
Patients (n = 118; median age 47 years; median Karnofsky performance status score: 80) were re-treated at a median of 28 months (range, 5-214 months) after initial radiation therapy. The median reirradiation dose was 41.4 Gy (range, 12.6-54.0 Gy) to a median lesion volume of 202 cm (range, 20-901 cm). The median cumulative (initial radiation and reirradiation combined) potential maximum brainstem dose was 76.9 Gy (range, 5.0-108.3 Gy) and optic apparatus dose was 56.0 Gy (range, 4.5-90.9 Gy). Of the patients, 56% received concurrent temozolomide, 14%, bevacizumab, and 11%, temozolomide plus bevacizumab; 19% had no chemotherapy. The planned reirradiation was completed by 90% of patients. Median OS from the completion of reirradiation was 9.6 months (95% confidence interval [CI], 7.5-11.7 months) for all patients and 14.0, 11.5, and 6.7 months for patients with initial grade 2, 3, and 4 glioma, respectively. On multivariate analysis, better OS was observed with a >24-month interval between radiation treatments (hazard ratio [HR]: 0.3; 95% CI, 0.2-0.5; < .001), reirradiation dose >41.4 Gy (HR: 0.6; 95% CI, 0.4-0.9; = .03), and gross total resection before reirradiation (HR: 0.6, 95% CI, 0.3-0.9; = .02). Radiation necrosis and grade ≥3 late neurotoxicity were both minimal (<5%). No symptomatic persistent brainstem or optic nerve/chiasm injury was identified.
Salvage reirradiation, even at doses >41.4 Gy in conventional fractionation, along with chemotherapy, was safe and well tolerated with meaningful survival duration. These data provide information that may be useful in implementing safe reirradiation treatments for appropriately selected patients and guiding future studies to define optimal reirradiation doses, maximal safe doses to critical structures, and the role of systemic therapy.
对于复发性胶质瘤的再程放疗,在缺乏最佳患者选择、剂量、分割方式及正常组织耐受性相关知识的情况下,仍存在争议。我们回顾性评估了复发性高级别胶质瘤采用常规分割再程放疗后的疗效和毒性,以及同步化疗的影响。
我们对2007年至2016年间因高级别胶质瘤复发而接受再程放疗的患者(包括初始为低级别胶质瘤的患者)进行了回顾性研究。疗效指标包括总生存期(OS)、生存预后因素及治疗相关毒性。
患者(n = 118;中位年龄47岁;中位卡氏功能状态评分:80)在初始放疗后中位28个月(范围5 - 214个月)接受再治疗。再程放疗的中位剂量为41.4 Gy(范围12.6 - 54.0 Gy),中位靶体积为202 cm³(范围20 - 901 cm³)。累积(初始放疗和再程放疗联合)潜在最大脑干剂量中位值为76.9 Gy(范围5.0 - 108.3 Gy),视路剂量中位值为56.0 Gy(范围4.5 - 90.9 Gy)。患者中,56%接受同步替莫唑胺治疗,14%接受贝伐单抗治疗,11%接受替莫唑胺加贝伐单抗治疗;19%未接受化疗。90%的患者完成了计划的再程放疗。所有患者再程放疗结束后的中位OS为9.6个月(95%置信区间[CI],7.5 - 11.7个月),初始为2级、3级和4级胶质瘤的患者分别为14.0个月、11.5个月和6.7个月。多因素分析显示,放疗间隔>24个月(风险比[HR]:0.3;95% CI,0.2 - 0.5;P <.001)、再程放疗剂量>41.4 Gy(HR:0.6;95% CI,0.4 - 0.9;P =.03)以及再程放疗前进行肉眼全切(HR:0.6,95% CI,0.3 - 0.9;P =.02)时,OS较好。放射性坏死和≥3级晚期神经毒性均较少(<5%)。未发现有症状的持续性脑干或视神经/视交叉损伤。
挽救性再程放疗,即使采用常规分割且剂量>41.4 Gy,并联合化疗,也是安全的且耐受性良好,生存期有意义。这些数据为对合适患者实施安全的再程放疗治疗以及指导未来研究确定最佳再程放疗剂量、关键结构的最大安全剂量和全身治疗的作用提供了有用信息。