Gandamihardja T A K, Soukup T, McInerney S, Green J S A, Sevdalis N
Chelmsford Breast Unit, Broomfield Hospital, Chelmsford, Essex, UK.
Centre for Implementation Science, Health Service and Population Research Department, King's College London, London, UK.
World J Surg. 2019 Feb;43(2):559-566. doi: 10.1007/s00268-018-4815-3.
Multidisciplinary team (MDT)-driven cancer care is a mandatory UK national policy, widely used globally. However, few studies have examined how MDT members make decisions as a team. We report a single-centre prospective study on team working within breast cancer MDT.
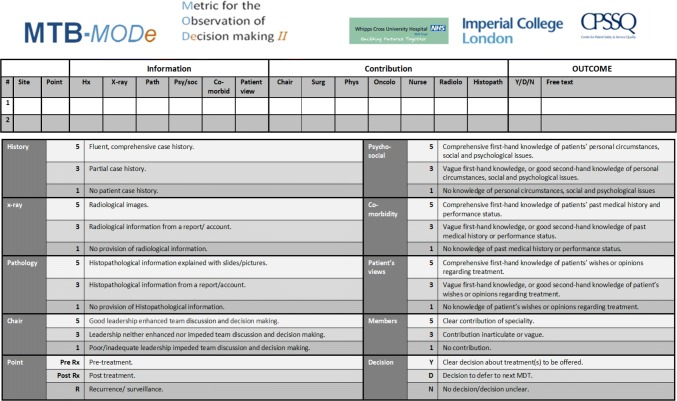
This was a prospective observational study of 10 breast MDT meetings (MDM). Trained clinical observer scored quality of presented information and disciplinary contribution to case reviews in real time, using a validated tool, namely Metric for the Observation of Decision-Making. Data were analysed to evaluate quality of team working.
Ten MDMs were observed (N = 346 patients). An average of 42 patients were discussed per MDM (range: 29-51) with an average 3 min 20 s (range: 31 s-9 min) dedicated to each patient. Management decision was made in 99% of cases. In terms of contribution to case reviews, breast care nurses scored significantly (p < 0.05) lower (M = 1.79, SD = 0.12) compared to other team members (e.g. surgeons, M = 4.65; oncologists, M = 3.07; pathologists, M = 4.51; radiologists, M = 3.21). Information on patient psychosocial aspects (M = 1.69, SD = 0.68), comorbidities (M = 1.36, SD = 0.39) and views on treatment options (M = 1.47, SD = 0.34) was also significantly (p < 0.05) less well represented compared to radiology (M = 3.62, SD = 0.77), pathology (M = 4.42, SD = 0.49) and patient history (M = 3.91, SD = 0.48).
MDT evaluation via direct observation in a meeting is feasible and reliable. We found consistent levels of quality of information coverage and contribution within the team, but certain aspects could be improved. Contribution to patient review resides predominantly with surgeons, while presented patient information is largely of biomedical nature. These findings can be fed to cancer MDTs to identify potential interventions for improvement.
多学科团队(MDT)驱动的癌症护理是英国一项强制性的国家政策,在全球广泛应用。然而,很少有研究探讨MDT成员如何作为一个团队做出决策。我们报告了一项关于乳腺癌MDT团队协作的单中心前瞻性研究。
这是一项对10次乳腺癌多学科诊疗会议(MDM)的前瞻性观察研究。经过培训的临床观察员使用一种经过验证的工具,即决策观察指标,实时对所呈现信息的质量以及各学科在病例讨论中的贡献进行评分。对数据进行分析以评估团队协作质量。
观察了10次MDM(N = 346例患者)。每次MDM平均讨论42例患者(范围:29 - 51例),平均每位患者用时3分20秒(范围:31秒 - 9分钟)。99%的病例做出了管理决策。在对病例讨论的贡献方面,与其他团队成员相比,乳腺护理护士的得分显著较低(p < 0.05)(M = 1.79,标准差 = 0.12),例如外科医生(M = 4.65)、肿瘤学家(M = 3.07)、病理学家(M = 4.51)、放射科医生(M = 3.21)。与放射学(M = 3.62,标准差 = 0.77)、病理学(M = 4.42,标准差 = 0.49)和患者病史(M = 3.91,标准差 = 0.48)相比,关于患者心理社会方面(M = 1.69,标准差 = 0.68)、合并症(M = 1.36,标准差 = 0.39)以及对治疗方案的看法(M = 1.47,标准差 = 0.34)的信息呈现也显著较少(p < 0.05)。
通过在会议中直接观察对MDT进行评估是可行且可靠的。我们发现团队内部信息覆盖质量和贡献水平较为一致,但某些方面仍可改进。对患者讨论的贡献主要来自外科医生,而所呈现的患者信息主要是生物医学性质的。这些发现可反馈给癌症MDT,以确定潜在的改进干预措施。